Manual coordination in DME billing works the same way it has for twenty years. A prior authorization request is assembled by hand, submitted to a payer portal by a billing coordinator, followed up by phone or fax, and tracked on a spreadsheet or in a Brightree workflow queue. An eligibility verification is run once at intake and not checked again until the claim is denied.
A denied claim sits in a queue until someone has time to classify it, draft an appeal, and resubmit. None of this is complicated. All of it is time-consuming, error-prone, and linear: it scales with headcount, not with order volume.
The DME AI stack replaces this coordination layer. It does not replace Brightree or NikoHealth; it sits on top of them. It does not replace the billing team; it changes what the billing team does. And it does not automate every decision; it automates 85 to 90 percent of cases that follow predictable patterns and routes the rest to a human reviewer with all relevant context already assembled.
This article is a technical and operational guide to building that stack: what the four layers are, how they connect, which agents handle which workflows, how the integration with Brightree and NikoHealth works at the API level, and what the implementation sequence looks like from readiness audit to full deployment. It is written for the COO who needs to make the investment case; the Director of Billing, who needs to validate the workflow logic; and the CTO who needs to sign off on the architecture.
What This Article Covers
- The four-layer architecture of the DME AI stack and what each layer does
- How to integrate Agentic AI workflows with Brightree and NikoHealth at the API level
- The six automation agents that replace manual billing coordination, and how they connect
- A platform-by-platform integration comparison: Brightree vs. NikoHealth vs. legacy systems
- Build vs. buy vs. partner: the honest tradeoffs for DME operators evaluating each path
- A phased implementation roadmap with gate criteria for each phase
- What the stack does not handle yet, and where the boundaries of automation sit
Why Does Manual Coordination Break Down as DME Operations Scale?
Manual coordination has three structural limits that automation removes.
Why Does Manual Billing Coordination Scale With Headcount Instead of Order Volume?
A billing coordinator processing prior authorizations manually can handle approximately 8 to 12 complex PAs per day, including documentation gathering, portal submission, and follow-up. Adding more orders requires adding more coordinators. The administrative cost per order is essentially fixed; it does not decline as volume grows. An AI prior auth agent on Brightree or NikoHealth processes prior authorizations continuously across all active orders simultaneously. Adding more orders does not require adding headcount.
How Do Manual Workflows Increase Denial Risk and Lost Revenue?
Manual workflows produce errors at predictable rates. A single eligibility check at intake misses mid-year plan changes, benefit exhaustions, and coordination-of-benefits shifts. A billing team at capacity on prior auth does not have time to work soft denials systematically. OIG’s 2023 DME billing compliance report found that the average DME provider writes off 6 to 12 percent of submitted claims; the majority are soft denials that are correctable on appeal. Manual coordination does not recover them because there is not enough time.
Why Do Manual Processes Create Compliance and Audit Challenges?
Manual documentation workflows produce inconsistent audit trails. When a TPE (Targeted Probe and Educate) or RAC (Recovery Audit Contractor) audit arrives, the billing team must reconstruct the documentation history for a sample of claims, which takes time, introduces errors, and reveals gaps that are difficult to explain. An AI stack with a proper audit log layer maintains a timestamped, attributable record of every action taken on every order, which makes audit response substantially faster and more defensible.
Table of Contents
Key Benchmarks
Prior auth processing: 6–9 days per complex order (manual), per the HFMA 2024 Revenue Cycle Benchmarking Report.
Soft denial write-off rate: 6–12% of submitted DME claims, per OIG 2023 DME billing compliance report.
Billing team capacity: 80–120 complex orders per billing FTE per month (manual baseline), per Clustox implementation data.
Admin overhead reduction: 47% across six workflows with full AI stack deployment, per Clustox implementation data.
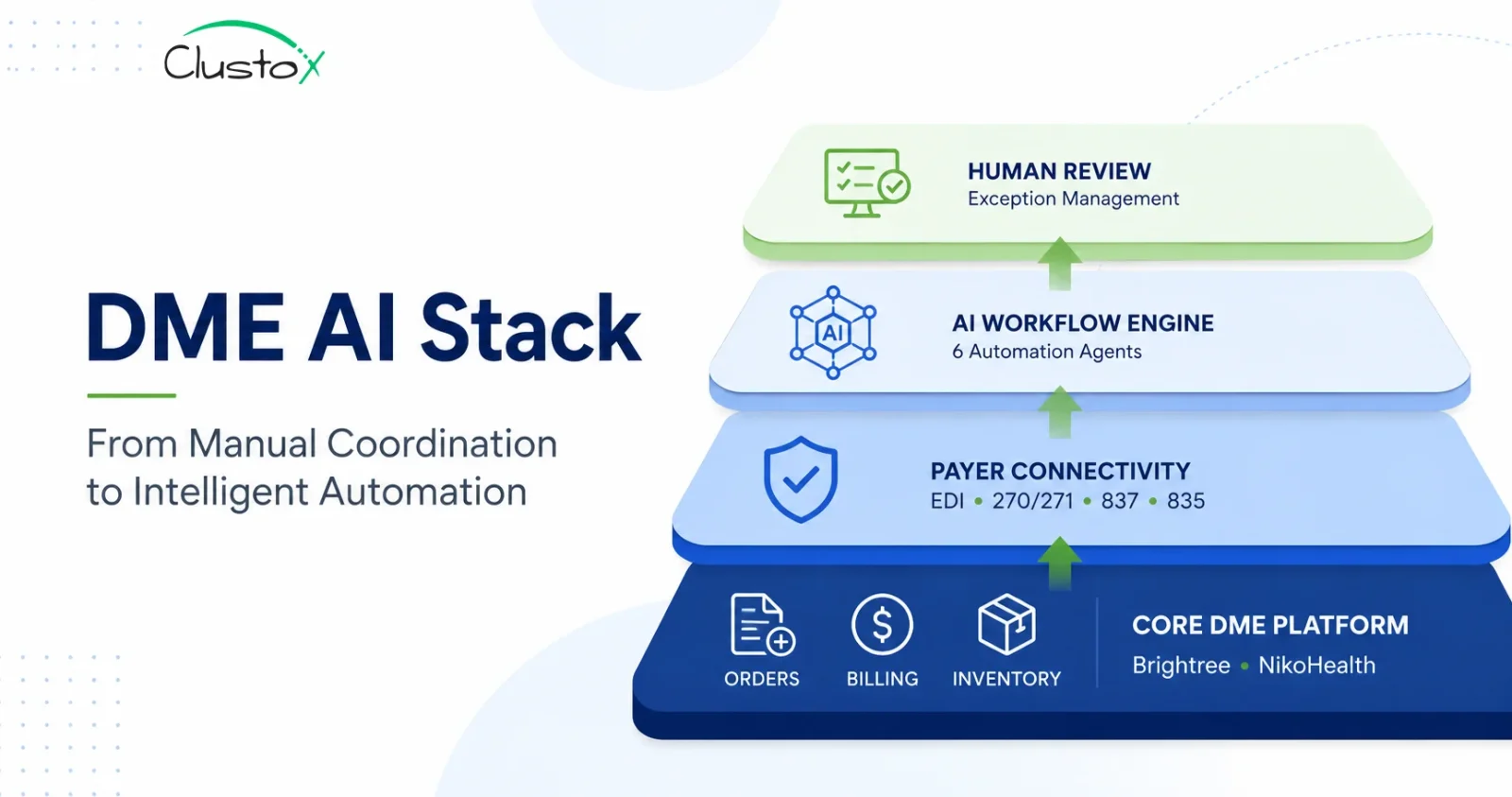
What Is the Four-Layer DME AI Stack Architecture?
The DME AI stack is not a single product. It is a layered architecture where each layer has a defined function and connects to the layers above and below it. Understanding the layers is essential for making good build-vs-buy decisions and for evaluating vendor claims.
Layer 1: The Core DME Platform (Data Foundation)
Brightree or NikoHealth is the data foundation. Patient records, orders, HCPCS codes, payer assignments, billing history, and inventory all live here. The AI stack reads from this layer continuously and writes results back into it. Every prior auth submission, every eligibility check result, every claim status, and every appeal outcome is recorded in the core platform as the system of record.
This is not a layer you build; it is a layer you integrate with. The quality of your API access to Brightree or NikoHealth is the single biggest determinant of how fast and how cheaply the AI layer integrates. NikoHealth’s modern REST API is the fastest integration path.
Brightree’s older API framework is well-tested and capable but requires more integration work. Legacy platforms, including TIMS and Bonafide, have limited API surfaces that make AI integration expensive and slow.
Layer 2: Payer Connectivity
The payer connectivity layer handles all EDI transactions: 270/271 eligibility queries, 837 claim submissions, and 835 remittance advice. This layer is typically provided through a clearinghouse such as Change Healthcare or Availity, supplemented by direct payer connections for high-volume relationships.
The AI eligibility agent uses this layer to run real-time 270/271 queries at three points in the order lifecycle. This approach is similar to modern automated insurance verification for DME workflows, where eligibility is validated continuously rather than only at patient intake.
The AI prior auth agent uses direct payer portal connections (via browser automation or API where available) in addition to EDI where the payer exposes it. This layer is mostly pre-built; your job is to confirm your clearinghouse relationships are in place and that your integration with Brightree or NikoHealth surfaces the right EDI endpoints for the AI agents to use.
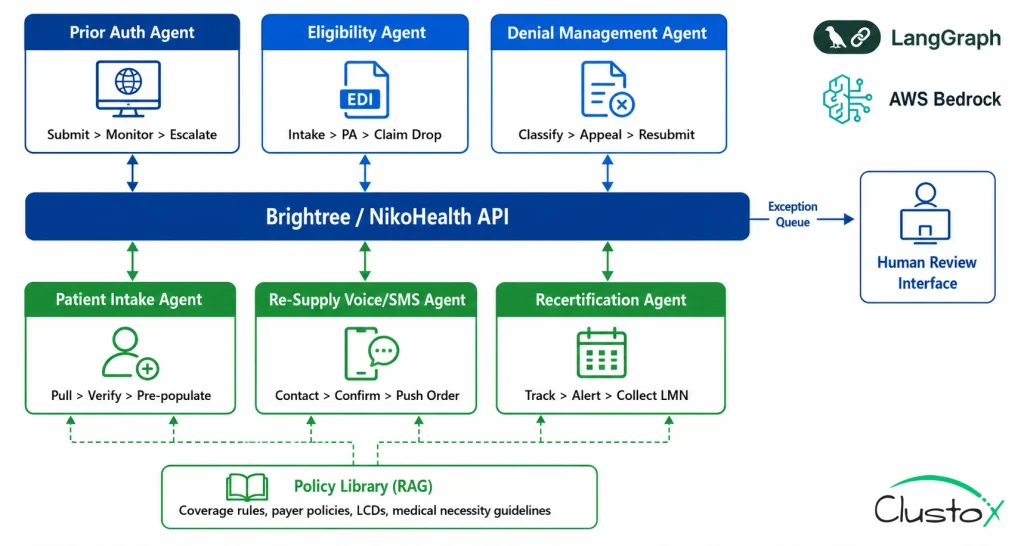
Layer 3: The Agentic AI Workflow Engine
This is the layer that replaces manual coordination. The AI workflow engine runs on LangGraph (for agent orchestration), deployed on AWS Bedrock (for HIPAA-compliant inference), with a RAG (Retrieval-Augmented Generation) pipeline providing access to the policy and rules library: CMS coverage criteria for each relevant HCPCS category, payer-specific PA requirements, LMN documentation standards, and denial pattern history.
The Prior Auth Agent automates documentation gathering, submission, status monitoring, and escalation workflows. Organizations looking to understand the operational impact of prior authorization automation for DME can explore how AI reduces approval turnaround times and manual workload.
- submits, monitors, and escalates prior authorization requests for E0601, E1390, K0001 to K0108, and other PA-required categories Prior Auth Agent:
- runs real-time 270/271 checks at intake, PA submission, and claim drop; flags benefit-limit proximity and COB issues. Eligibility Agent:
- Advanced denial management software for DME helps organizations identify recurring denial patterns, automate appeals, and improve recovery rates across payer categories.
- pulls referral orders, verifies insurance, confirms HCPCS qualification, and pre-populates Brightree or NikoHealth order records. Patient Intake Agent:
- contacts CPAP patients via voice and SMS at re-supply intervals; pushes confirmed orders back to the platform. Re-Supply Voice/SMS Agent:
- tracks oxygen recertification schedules, alerts referring physicians, and collects updated LMN documentation. Recertification Agent:
Each agent is goal-directed, not rules-based. It does not follow a fixed script; it pursues a defined outcome (get the PA approved, confirm the patient’s coverage, recover the denied claim) and adapts to non-standard responses within defined parameters. Genuine exceptions, situations where the agent cannot proceed without human judgment, are routed to Layer 4 with full context.
Layer 4: The Human Review Interface
The human review layer is where the billing team works in an AI-first operation. Instead of processing every order, they review an exception queue: prior authorization requests that require peer-to-peer escalation, eligibility situations that require manual investigation, appeal drafts that need a human signature, and recertification cases where the referring physician has not responded.
The interface surfaces every exception with the relevant context already assembled by the AI agent: the order record, the payer response, the recommended action, and the documentation that supports it. A billing coordinator reviewing an exception spends 5 to 15 minutes on it, not 45 minutes. This layer also maintains the full audit log for TPE and RAC audit defense: every automated action, every payer response, and every escalation decision is timestamped and attributable.
What Results Can DME Providers Expect From a Full AI Stack?
The table below maps every component of the DME AI stack by layer, function, tooling, and integration point. Use this as a reference when evaluating vendor proposals or designing your own build.
| Stack Layer | Component | Function | Tools / Platforms | Integration Point |
|---|---|---|---|---|
| Layer 1: Data Foundation | Core DME Platform | Patient records, orders, HCPCS coding, billing, inventory | Brightree, NikoHealth | AI reads/writes via API |
| Layer 1: Data Foundation | Payer Connectivity | 270/271 eligibility, 837 claims, 835 remittance via EDI | Change Healthcare, Availity | EDI clearinghouse layer |
| Layer 2: AI Orchestration | Workflow Engine | Goal-directed agent orchestration across multi-step tasks | LangGraph, AWS Bedrock | Sits atop DME platform API |
| Layer 2: AI Orchestration | Policy + Rules Library | CMS coverage criteria, payer-specific PA rules, LMN requirements | CMS.gov, payer portals, RAG | Knowledge base for agents |
| Layer 2: AI Orchestration | Document Intelligence | LMN completeness checks, ICD-10 mapping, HCPCS documentation | LLM, RAG pipeline | Order intake and PA validation |
| Layer 3: Automation Agents | Prior Auth Agent | Submit, monitor, and escalate prior authorization requests | LangGraph + Brightree API | Payer portal / fax API |
| Layer 3: Automation Agents | Eligibility Agent | Real-time 270/271 checks at intake, PA submission, claim drop | NikoHealth API + clearinghouse | Payer EDI layer |
| Layer 3: Automation Agents | Denial Management Agent | Classify, draft appeals, resubmit; feed patterns upstream | LLM + Brightree/NikoHealth API | Payer appeal portals |
| Layer 3: Automation Agents | Re-Supply Voice/SMS Agent | Outbound CPAP patient outreach; push confirmed orders back | Voice AI, SMS platform | Brightree/NikoHealth fulfillment |
| Layer 3: Automation Agents | Recertification Agent | Oxygen cert schedule tracking, physician alerts, doc collection | Brightree/NikoHealth + alerts | Referring physician workflow |
| Layer 4: Human Review Layer | Exception Queue Interface | Surfaces AI-flagged exceptions with context for human review | Custom UI / Brightree views | Billing team touchpoint |
| Layer 4: Human Review Layer | Audit Trail Logger | Timestamped log of every automated action for TPE/RAC defense | AWS CloudWatch / native logs | Compliance and audit layer |
Which DME Platform Is Best for AI Integration: Brightree, NikoHealth, or Legacy Systems?
The AI stack works on top of your existing DME platform. The platform determines how fast you can integrate, how deep the integration goes, and how much it costs. The comparison below is based on production integrations across Brightree and NikoHealth environments, supplemented by integration assessment data for legacy platforms.
| Integration Criterion | Brightree | NikoHealth | TIMS / Legacy |
|---|---|---|---|
| API architecture | Older SOAP/REST hybrid; capable, tested | Modern REST; fastest integration path | Limited; often requires middleware |
| AI integration difficulty | Medium; established integration patterns | Low; clean API surface, well-documented | High; significant integration cost |
| Data read access (orders) | Full via integration partner framework | Full via native REST API | Partial; often manual export required |
| Data write access (results) | Full; AI writes status back to orders | Full; native API write support | Limited; may require workarounds |
| Prior auth workflow hooks | Configurable; API-accessible workflow triggers | Configurable; modern event hooks | Limited; mostly rules-based native only |
| Eligibility API integration | Via clearinghouse (Change HC, Availity) | Native + clearinghouse support | Clearinghouse only; less configurable |
| HIPAA BAA compatibility | Yes; supports AWS Bedrock BAA chain | Yes; supports BAA with cloud providers | Case by case; verify before committing |
| Implementation timeline | 8–12 weeks for PA + eligibility | 6–10 weeks for PA + eligibility | 16–24+ weeks; often requires migration |
| Recommended for AI-first ops? | Yes, for existing large Brightree shops | Yes, especially for new or migrating ops | No; migrate to Brightree or NikoHealth first |
What This Means in Practice
If you are on Brightree, your integration path is well-established. Expect 8 to 12 weeks for prior auth and eligibility automation. The API framework is capable, and the integration patterns are documented. The main variables are your API credential configuration and the quality of your order data.
If you are on NikoHealth, you have the fastest integration path available. NikoHealth’s REST API is designed for external integration. Expect 6 to 10 weeks for prior auth and eligibility automation. The data model is cleaner, which reduces the transformation work between the platform and the AI layer.
If you are on TIMS, Bonafide, or another legacy system, the honest answer is that AI integration complexity on legacy platforms typically costs more and takes longer than a platform migration to NikoHealth followed by AI integration. A 48-hour AI Readiness Audit will tell you the cost-benefit comparison for your specific situation before you commit to either path.
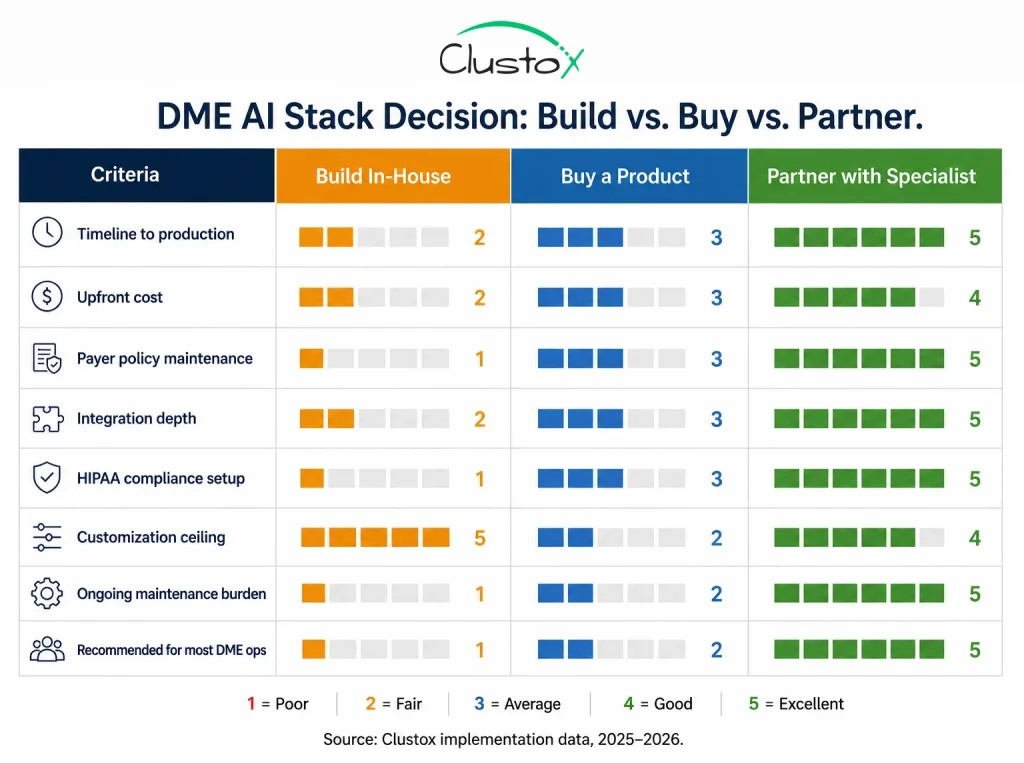
Should DME Providers Build, Buy, or Partner for AI Automation?
Every DME operator evaluating an AI stack faces the same decision: build it in-house, buy an off-the-shelf product, or partner with a specialist. Each path has a different cost structure, timeline, and risk profile.
The table below maps the honest tradeoffs across eight criteria.
| Decision Criterion | Build In-House | Buy a Vendor Product | Partner with Specialist |
|---|---|---|---|
| Typical timeline to live workflow | 9–18 months | 3–6 months (if well-configured) | 6–12 weeks (Clustox pattern) |
| Upfront cost | High (eng team, infra, compliance) | Medium (licensing + configuration) | Low to medium (fixed-price audit first) |
| Ongoing cost | High (maintenance, payer updates) | Medium (license + customisation limits) | Low (partner manages payer updates) |
| Payer policy library maintenance | Your responsibility; hard to keep current | Vendor maintains; may lag | Partner maintains continuously |
| HIPAA BAA and compliance setup | Your responsibility; complex | Vendor handles; verify BAA chain | Partner handles with your infra sign-off |
| Integration depth (Brightree/Niko) | Deep if you build it right; rarely is | Varies; often limited by product scope | Deep by design; primary deliverable |
| Exception handling customisation | Full control; high maintenance | Limited by product roadmap | Co-designed per your payer mix |
| Best for | Operators with dedicated eng teams | Operators wanting off-shelf speed | Operators wanting depth without the build |
1. The Build Path
Building in-house gives you full control over integration depth, agent behavior, and payer policy customization. It also gives you full responsibility for every layer: HIPAA compliance architecture, payer portal integrations, LMN documentation standards, denial pattern libraries, and ongoing maintenance as payer policies change. DME operators with a dedicated engineering team and a 12 to 18 month timeline can build a capable stack. Most do not have that combination.
2. The Buy Path
Off-the-shelf DME AI products are increasingly available, but the category is early. Most vendor products that claim AI automation for DME are closer to rules-based workflow tools with an AI marketing layer.
The test is simple: ask the vendor to demonstrate a complete prior authorization cycle, from order creation to payer approval, with no human touchpoints, on a live Brightree or NikoHealth environment. If they cannot, the product is not what it claims to be. Licensing costs are medium, but the ceiling on customization limits how deeply the product adapts to your specific payer mix.
3. The Partner Path
Partnering with a specialist who builds Agentic AI workflows on top of your existing Brightree or NikoHealth platform is the fastest path to production-depth automation for most DME operations.
The key difference from buying a product is that the implementation is designed around your payer mix, your HCPCS categories, and your exception patterns, not a generic product configuration. The upfront cost is lower than building, the timeline is faster than both alternatives, and the payer policy library is maintained by the partner rather than your team.
What Are the Real Tradeoffs Between Building, Buying, and Partnering?
The roadmap below covers seven phases from initial readiness assessment through full six-agent deployment. Each phase has a defined set of activities, a realistic timeline, and a gate criterion that must be met before the next phase begins. This sequencing is not arbitrary; each phase builds the foundation the next phase depends on.
| Phase | Activities | Timeline | Gate Criteria to Proceed |
|---|---|---|---|
| Phase 0: Readiness Audit | Map workflow friction points; confirm Brightree or NikoHealth API access; data quality review; payer priority analysis; document current baseline metrics | Days 1–2 | API access confirmed; baseline metrics documented; top 3 workflows identified |
| Phase 1: Stack Design | Define agent architecture; select infrastructure (AWS Bedrock); confirm HIPAA BAA; map payer policy library for top 10 payers; design exception routing logic | Weeks 1–2 | BAA signed; policy library seeded; architecture signed off |
| Phase 2: Prior Auth Agent | Build and deploy PA agent on Brightree or NikoHealth; run parallel with manual for 2–4 weeks; validate accuracy on 200+ orders; cut over to AI-primary | Weeks 3–9 | 85%+ PA automation rate; error rate below manual baseline |
| Phase 3: Eligibility Agent | Deploy 3-point eligibility verification at intake, PA submission, and claim drop; monitor eligibility denial rate weekly; tune benefit-limit flagging | Weeks 10–13 | Eligibility denial rate tracking downward within 30 days |
| Phase 4: Denial Management | Deploy denial classification and appeal agent; establish appeal success rate baseline; activate upstream pattern feedback to PA and eligibility agents | Weeks 14–20 | 18%+ of previously written-off denials recovered within 60 days |
| Phase 5: Intake + Re-Supply | Deploy patient intake qualification agent; activate CPAP re-supply voice and SMS agents; set re-supply interval rules per product category | Months 5–6 | Intake time below 15 min; re-supply capture rate 30%+ above baseline |
| Phase 6: Recertification | Deploy oxygen recertification tracking and physician alert workflow; integrate with LMN collection process; set 30-day and 14-day alert thresholds | Month 6+ | Zero missed recertification windows in first 90-day period |
What Is the Recommended Roadmap for Implementing a DME AI Stack?
The metrics below reflect Clustox implementations across DME clients on Brightree and NikoHealth, validated against HFMA 2024, AAHomecare 2024, and OIG 2023 benchmarks. Results vary by payer mix, order volume, and existing workflow maturity.
| Metric | Manual Baseline | AI Stack Result | Source |
|---|---|---|---|
| Prior auth turnaround | 6–9 days per complex order | Under 48 hours | HFMA 2024; Clustox data |
| PA automation rate | 0% (fully manual) | 85–92% of routine PAs | Clustox implementation data |
| Eligibility denial rate | Baseline (single-check intake) | Down 15–22% | Clustox implementation data |
| Soft denial write-off rate | 6–12% of submitted claims | 18–27% recovered in 90 days | OIG 2023; Clustox data |
| Patient intake time | 45–60 min per new patient | 8–12 min (AI-assisted) | Clustox implementation data |
| CPAP re-supply capture | 30–40% patient reach (phone) | 65–75% reach (voice + SMS) | Clustox implementation data |
| Missed oxygen recertifications | 3–8% annually (manual tracking) | Near zero with automation | CMS MLN; Clustox data |
| Overall admin overhead | Baseline | 47% reduction | Clustox implementation data |
| Order capacity per billing FTE | 80–120 complex orders/month | 200–240 orders/month | Clustox implementation data |
What HIPAA Requirements Must a DME AI Stack Meet?
HIPAA compliance in an AI stack is not a feature of the AI model. It is an architecture requirement. Every component that processes, stores, or transmits Protected Health Information (PHI) must operate under a signed Business Associate Agreement (BAA) with the covered entity (the DME provider).
1. BAA Chain Requirements
The BAA chain for a typical DME AI stack runs as follows:
DME provider signs BAA with Brightree or NikoHealth (already in place for most operators); DME provider or implementation partner signs BAA with AWS (for AWS Bedrock inference); DME provider or implementation partner signs BAA with any third-party voice or SMS platform used for re-supply outreach. AWS Bedrock, Azure OpenAI Service, and GCP Vertex AI all offer BAA-eligible environments. HHS.gov publishes current guidance on HIPAA BAA requirements at hhs.gov/hipaa.
2. Data Residency and Encryption
PHI must be encrypted in transit (TLS 1.2 or higher) and at rest (AES-256 or equivalent). For AWS Bedrock deployments, this is handled by the service by default; confirm your key management configuration. Audit logs must be retained per HIPAA’s six-year minimum retention requirement. AWS CloudWatch or equivalent logging infrastructure handles this for cloud-deployed stacks.
3. Minimum Necessary Standard
AI agents must operate on the minimum necessary PHI to perform their function. The prior authorization agent does not need payment history; the resupply agent does not need full clinical records. Designing data access scopes per agent is both a HIPAA compliance requirement and a good security practice. Document your data access decisions in your HIPAA Security Rule risk analysis.
What Can the DME AI Stack Automate, and What Still Requires Human Review?
The DME AI stack described in this article is production-tested and delivering the results in the metrics table above. It is not a complete automation solution without boundaries.
Here is where the current limits sit.
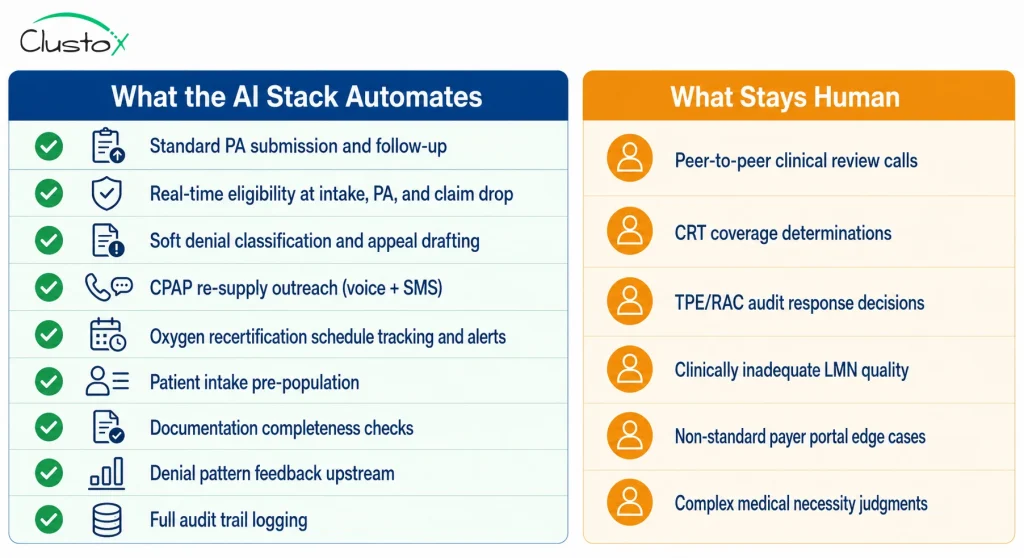
1. Non-Standard Payer Portal Interfaces
AI agents perform most reliably on payer portals with consistent, documented interfaces. Some regional Medicare Advantage plans and Medicaid managed care organizations use non-standard portals that require custom browser automation or a manual fallback path. Expect 10 to 20 percent of your payer mix to require a manual fallback at initial deployment, declining as the agent learns each portal over the first 60 to 90 days.
2. Complex Rehab Technology Prior Authorization
For CRT categories, including K0800 through K0899 (custom power wheelchairs), complex seating systems, and custom orthotics, documentation requirements are individualized and payer-specific in ways that do not generalize cleanly to automated agents.
The PA agent assists with documentation completeness checks and submission logistics, but the clinical coverage determination requires a trained specialist. Do not fully automate CRT prior authorization without a human clinical reviewer in the exception queue.
3. Peer-to-Peer Review Escalation
When a payer denies a prior authorization and requests a peer-to-peer review between the DME provider’s clinical staff and the payer’s medical director, the AI agent identifies and routes the escalation. The actual peer-to-peer call remains a human responsibility. The agent can prepare the documentation package and schedule context, but the clinical conversation is out of scope.
4. TPE and RAC Audit Response Decisions
AI can assemble the documentation package for a TPE (Targeted Probe and Educate) or RAC (Recovery Audit Contractor) audit response: pulling claim records, organizing supporting clinical documentation, and formatting the response per contractor requirements. The substantive decision about how to respond, especially for contested findings, requires human review and in material cases qualified healthcare counsel. Automate the assembly; keep the decision human.
5. LMN Content Quality
The documentation agent checks whether a Letter of Medical Necessity is present and whether it contains the required elements for the relevant HCPCS category. It cannot improve a clinically inadequate LMN. Providers with weak referral source relationships will see elevated PA exception rates regardless of automation quality. The stack amplifies documentation input quality; it does not substitute for it.
Is Your DME Organization Ready for AI Workflow Automation?
Before committing to a DME AI stack implementation, evaluate your organization’s readiness across platform access, compliance, payer connectivity, data quality, operational processes, and team preparedness.
The checklist below helps identify potential blockers before they become expensive implementation delays.
| Criteria | Questions to Ask | Status |
|---|---|---|
| API Access | Do we have API documentation and sandbox credentials for Brightree or NikoHealth? Can the implementation team access orders, claims, eligibility data, and patient records through approved APIs? | ☐ |
| HIPAA Compliance | Have we identified every system that will process PHI? Are Business Associate Agreements (BAAs) in place with AWS Bedrock, voice providers, SMS vendors, and other infrastructure partners? | ☐ |
| Payer Readiness | Have we documented our top 10 payers by claim volume and prior authorization burden? Do we know which payers require custom integrations or manual fallback workflows? | ☐ |
| Baseline Metrics | Have we measured current prior authorization turnaround times, eligibility denial rates, soft-denial write-offs, and orders processed per billing FTE? | ☐ |
| Data Quality | Have we reviewed a recent sample of Brightree or NikoHealth records for missing insurance data, documentation gaps, coding errors, and incomplete patient information? | ☐ |
| Implementation Sequence | Is there agreement on the deployment order: Prior Authorization → Eligibility Verification → Denial Management → Intake → Re-Supply → Recertification? | ☐ |
| Success Criteria | Have measurable gate criteria been defined for every implementation phase, including automation targets, error thresholds, and operational KPIs? | ☐ |
| Team Readiness | Has the billing team been informed about workflow changes? Are training sessions, escalation paths, and exception-review responsibilities documented before go-live? | ☐ |
Recommendation: Complete this checklist before selecting a vendor, approving implementation budgets, or beginning AI workflow deployment.
Frequently Asked Questions
What is the difference between a DME AI stack and rules-based billing automation?
Rules-based automation executes fixed if-then logic on predictable inputs. It handles structured, repetitive tasks but cannot adapt to non-standard payer responses, navigate portal interfaces that change between sessions, or make contextual decisions about documentation completeness. Agentic AI in a properly built DME stack is goal-directed: the prior auth agent's goal is to get the authorization approved, and it pursues that goal through whatever steps the payer requires, including handling non-standard responses. Rules-based tools typically automate 40 to 60 percent of prior auth submissions; Agentic AI workflows consistently reach 85 percent or higher within 90 days of deployment.
Does the DME AI stack replace Brightree or NikoHealth?
No. The DME AI stack integrates with Brightree or NikoHealth via API; it does not replace them. Brightree and NikoHealth remain the system of record for all patient records, orders, billing, and inventory. The AI stack reads from the platform continuously and writes results back into it. Every automated action is recorded in the core platform as an audit trail. The stack adds an automation and coordination layer on top of the platform your team already uses.
How does the AI stack integrate with Brightree specifically?
The Brightree integration uses Brightree's API framework, which provides read and write access to orders, patients, claims, and workflow queues. The prior auth agent reads order data and LMN documentation, submits PA requests via payer portal or fax API, and writes authorization numbers and status updates back to the relevant order records in Brightree. The eligibility agent queries the clearinghouse through Brightree's EDI connections and flags eligibility issues in the order workflow. Implementation typically takes 8 to 12 weeks for prior auth and eligibility automation on Brightree, assuming API credentials are confirmed at project start.
Is the DME AI stack HIPAA compliant?
A properly architected DME AI stack is HIPAA compliant, but compliance is an architecture requirement, not a product feature. All AI processing of Protected Health Information must occur under signed HIPAA Business Associate Agreements with each infrastructure component: the DME platform (Brightree or NikoHealth), the AI inference provider (AWS Bedrock, Azure OpenAI, or GCP Vertex AI), and any third-party voice or SMS platform. PHI must be encrypted in transit and at rest. Audit logs must be retained for a minimum of six years per HIPAA requirements. HHS guidance on BAA requirements is available at hhs.gov/hipaa.
Should I build the DME AI stack in-house, buy a product, or partner with a specialist?
The build path requires a dedicated engineering team and 12 to 18 months; most DME operators do not have that combination. The buy path is faster but limited by product scope, and most off-the-shelf DME AI products are closer to rules-based tools than true Agentic AI systems. The partner path is the fastest route to production-depth automation for most operations: an experienced implementation partner designs the stack around your payer mix and HCPCS categories, maintains the payer policy library, and delivers a working prior auth and eligibility automation in 8 to 12 weeks. The 48-hour AI Readiness Audit maps your specific situation and produces a cost-benefit analysis for all three paths before you commit to any of them.
How long does it take to build and deploy the full DME AI stack?
Phase 0 (readiness audit) takes two days. Phase 1 (stack design and BAA setup) takes one to two weeks. Phase 2 (prior auth agent) takes six to seven weeks including parallel testing. Phase 3 (eligibility) adds three to four weeks. Phase 4 (denial management) adds four to six weeks. Phases 5 and 6 (intake, re-supply, recertification) complete the deployment in Months 5 and 6. Full deployment from signed contract to all six agents live is typically four to six months for operations on Brightree or NikoHealth with confirmed API access and clean data. Legacy platform environments add four to eight weeks.
What results should I expect from the full AI stack?
Based on Clustox implementation data across Brightree and NikoHealth environments: prior auth turnaround drops from 6 to 9 days to under 48 hours for standard HCPCS categories; 85 to 92 percent of routine PAs are automated end to end; eligibility-driven soft denials drop 15 to 22 percent; 18 to 27 percent of previously written-off soft denials are recovered within 90 days; CPAP re-supply patient reach improves from 30 to 40 percent (phone only) to 65 to 75 percent (voice plus SMS); and overall administrative overhead drops 47 percent. Billing team order capacity per FTE typically increases from 80 to 120 orders per month to 200 to 240 orders per month.
What are the most common reasons DME AI stack implementations fail?
The four most common failure modes are skipping the readiness audit and discovering API access or data quality blockers during the build phase; attempting to automate all six workflows simultaneously rather than sequentially; launching the prior auth agent without a complete, current payer policy library for the operation's top payers; and failing to brief and train the billing team before cutover, which creates resistance and inflates the exception rate in the first 30 days. All four are preventable with proper upfront planning.
Can the DME AI stack handle Medicare Advantage prior authorization?
Yes, for the major Medicare Advantage plans, including UnitedHealthcare, Humana, CVS/Aetna, and Elevance, with established integration paths on their PA portals. For smaller regional MA plans with non-standard portal interfaces, expect a manual fallback path at initial deployment. The agent learns non-standard portals over time, and most are mappable within the first 60 to 90 days of operation. Confirm payer-specific coverage with your implementation partner before go-live; this is one of the most important pre-implementation questions.
Conclusion
The DME AI stack described in this article is not a future-state vision. It is a proven architecture that is already helping DME providers automate prior authorizations, eligibility verification, denial management, patient intake, and recertification workflows. With Brightree and NikoHealth serving as the system of record, AI adds an intelligent coordination layer that reduces manual effort while improving operational efficiency.
The organizations seeing the strongest results are not necessarily the ones with the most resources; they are the ones that implement automation in the right sequence and focus on high-impact workflows first. Prior authorization, eligibility verification, and denial management create the foundation for broader automation across the revenue cycle. As routine work shifts to AI agents, billing teams can focus their time on the exceptions that require human expertise, leading to faster reimbursements, higher productivity, and lower administrative overhead.
For DME providers evaluating their next step, the priority should not be whether AI is ready—it is whether your workflows are ready to take advantage of it. Working with an experienced partner for AI development services can help accelerate implementation, reduce integration risk, and create a roadmap tailored to your payer mix, operational goals, and technology stack.
The opportunity is no longer theoretical. The technology exists, the implementation patterns are proven, and the potential impact on revenue cycle performance is measurable. The next move is deciding where to start.
Ready to Modernize Your DME Operations?
Discover where AI can reduce manual work, accelerate reimbursements, and improve operational efficiency.