
Most DME billing software generates errors because it relies on static rules, manual data entry, and disconnected workflows. AI-powered DME billing software reduces claim errors by automating eligibility checks, prior authorization, and documentation validation before a claim is ever submitted, cutting denial rates and shortening the revenue cycle.
Claim denials are expensive. Not just in the dollar amount you lose when a payer rejects a claim, but in the staff hours spent working that denial, the delayed cash flow, and the slow erosion of your team’s bandwidth.
For Directors of Billing and DME owners, the problem is rarely carelessness. It’s the software. Conventional DME billing platforms were built to record transactions, not to prevent errors. They accept incomplete data. They miss eligibility gaps. They send claims that were never going to get paid.
In 2026, that is no longer acceptable when there is a better option. AI-powered DME billing software does something fundamentally different: it works upstream, catching problems before they become denials. This guide walks you through where errors originate, what modern AI actually does to stop them, and how to evaluate whether your current platform is costing you more than you realize.
What Makes DME Billing Software Error-Prone in the First Place?
To understand why AI helps, you first need to understand why errors happen so consistently with standard DME billing software.
DME billing is not straightforward. A single claim can touch eligibility verification, prior authorization, HCPCS coding, documentation compliance, and payer-specific rule sets, all before it leaves your office. Each step is an opportunity for a mistake.
Standard billing platforms process what you give them. They do not ask whether what you gave them is complete or accurate. If a billing specialist enters the wrong modifier, the software sends the claim with the wrong modifier. If a prior auth has expired, the software sends the claim anyway.
Table of Contents
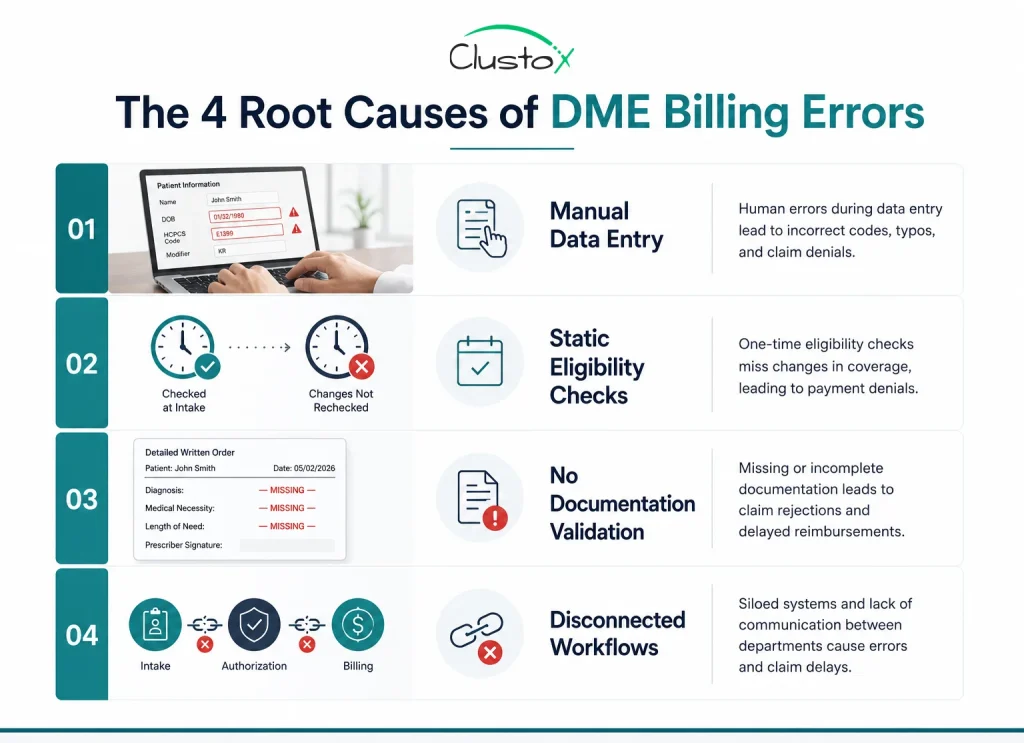
The structural problems fall into four categories:
Which Billing Errors Cost DME Providers the Most Money?
Not all errors carry the same cost. Some produce outright denials. Others create partial payments or lengthy appeals that pull your team away from current claims.
The highest-cost errors in DME billing tend to cluster around three areas:
Prior authorization errors
Prior auth is the single biggest source of preventable denials in DME. Missing authorizations, expired authorizations, and authorizations that do not match the ordered item account for a significant portion of claim rejections.
Manual prior auth workflows are slow by design. When a billing specialist has to call payers, track auth status in a spreadsheet, and manually cross-reference the authorized code against the claim, errors compound. Agentic AI can monitor authorization status continuously and flag mismatches before submission.
Eligibility and benefits verification gaps
Eligibility verified at intake does not mean eligibility is still valid at delivery. Patient insurance status changes. Coverage details shift. A verification run three weeks before delivery may not reflect the patient’s current benefits.
Platforms that check eligibility once and cache the result expose you to denials that were entirely preventable with a second check closer to the claim date.
HCPCS coding and modifier errors
HCPCS codes for DME are specific and modifier-sensitive. A missing KX modifier on a diabetic supply claim, or the wrong rental versus purchase indicator on a power wheelchair, will produce a denial or a significant underpayment.
Standard billing software accepts whatever modifier the specialist enters. AI-powered platforms cross-reference the ordered item, the diagnosis, the coverage criteria, and the payer’s specific rules to surface likely coding errors before submission.
| Error Type | Typical Consequence |
|---|---|
| Prior authorization mismatch | Outright denial, full rework required |
| Stale eligibility check | Claim denial, patient balance disputes |
| Missing or wrong HCPCS modifier | Denial or significant underpayment |
| Incomplete LMN documentation | Audit risk, post-payment recoupment |
| Wrong place-of-service code | Rejection, delayed payment cycle |
How Does AI Reduce Claim Errors in DME Billing Software?
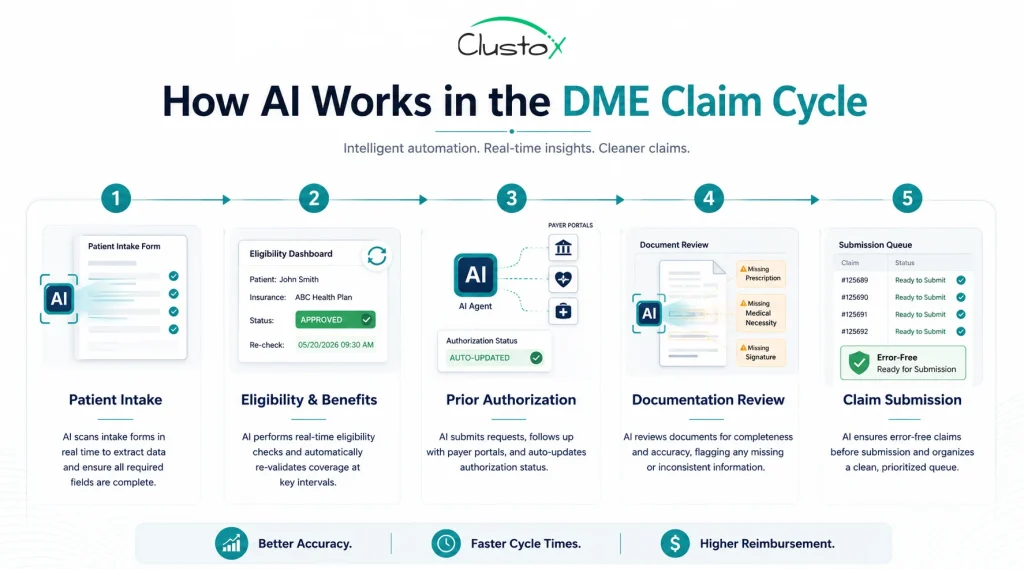
AI does not replace your billing team. It gives them better information earlier. The practical difference between a standard platform and an AI-integrated one comes down to when problems surface: before submission or after denial.
Automated prior authorization tracking
AI agents can connect directly to payer portals and monitor authorization status in real time. When an auth is about to expire, or when an authorized code does not match the item being ordered, the system flags it before the claim goes out.
Continuous eligibility verification
Rather than a one-time check at intake, AI can run eligibility queries closer to delivery and flag changes automatically. This is particularly important for recurring supply patients, where a coverage lapse may not surface until the claim is denied months later.
Documentation gap detection
AI models trained on payer LCD requirements and CMS coverage criteria can scan documentation for missing or insufficient fields before a claim is submitted. A letter and certificate of medical necessity that lacks a required diagnosis code, or a delivery receipt missing a required patient signature, can be flagged in real time rather than discovered during an audit.
Denial pattern analysis
Over time, AI learns from your denial history. If a specific payer consistently rejects claims with a particular coding pattern, the system can flag similar patterns on future claims. This is one area where AI compounds in value: the longer it runs, the more specific its predictions become.
What Should You Look for in DME Billing Software with AI Features?
Not every platform that mentions AI is actually using it in a meaningful way. Some vendors apply AI to cosmetic features like dashboard analytics while leaving the actual claim-generation workflow untouched.
Here is what matters when you are evaluating platforms:
- Pre-submission claim scrubbing with payer-specific rule sets, not just generic CMS edits
- Real-time eligibility checks that run multiple times in the claim cycle, not just once at intake
- Prior auth status monitoring with automated expiration alerts
- Documentation validation against LCD and payer-specific coverage criteria
- Denial analytics that feed back into the submission workflow
- Integration with your existing DME software ecosystem (Brightree, NikoHealth, TIMS, Fastrack)
- Audit trail and compliance logging for HIPAA and accreditation requirements
What Does a High Denial Rate Actually Signal About Your Billing Software?
A denial rate above a certain threshold is not just a billing team problem. It is a systems problem. If your team is spending a material portion of their week working denials rather than submitting clean claims, the software is not doing its job.
A useful way to think about it: every denial that reaches your desk is a claim the software let through when it should have flagged it. Your billing specialists are performing error correction that the platform should have caught automatically.
When you calculate the true cost of a denial, you have to include more than the claim value. You have to include:
- Staff time to identify the denial and root cause
- Time to gather additional documentation or authorizations
- Time to resubmit, and in many cases, to appeal
- The cost of delayed cash flow during the rework period
- The portion of denials that are never successfully recovered
Can AI Billing Software Integrate with Existing DME Workflows?
This is one of the most practical questions to ask before committing to any platform change, and the answer depends on how your current operation is structured.
Most DME billing operations have a mix of software: a core platform like Brightree or TIMS, a separate EHR or referral intake tool, possibly a standalone eligibility verification tool, and some combination of payer portals that billing staff access manually.
AI billing tools that work best in this environment are designed to integrate into existing workflows rather than replace them wholesale.
There are three integration models worth understanding:
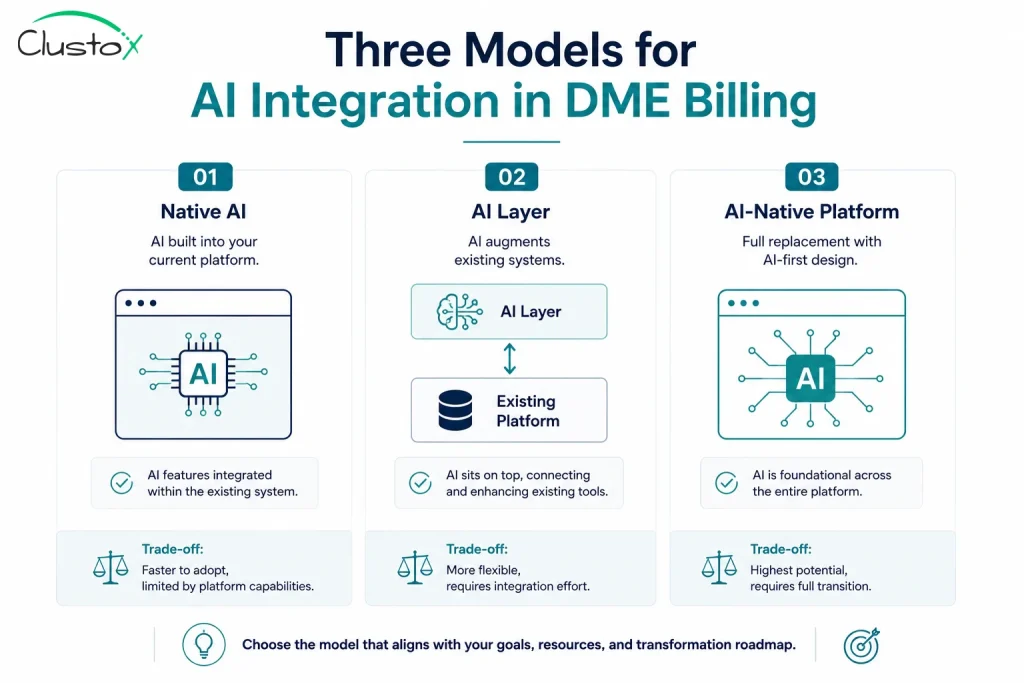
Native AI within your current platform
If your existing DME billing software is actively adding AI capabilities, you may be able to activate new features without a platform switch. Brightree and NikoHealth have both been investing in AI-assisted workflows. The limitation is that native AI is constrained by what the platform vendor prioritizes, and rollouts are incremental.
AI layer on top of existing systems
Some AI providers build a layer that sits on top of your existing billing platform, pulling data from it and pushing recommendations back without a full replacement. This approach preserves your current setup while adding intelligence at specific points in the workflow. It is lower disruption but requires careful API mapping.
Full AI-native platform replacement
For operations that are already planning a platform migration, choosing an AI-native DME billing platform from the start is often cleaner than retrofitting. The trade-off is higher implementation cost and a longer transition period. For a practice doing significant monthly billing volume, the math often favors this route over a medium-term horizon.
What Are the Realistic Limits of AI in DME Billing Software?
AI in DME billing is genuinely useful. It is also not a complete solution to every billing challenge you face. Being clear on what it does and does not do will help you set accurate expectations before a purchase decision.
What AI does well
- Detecting data entry errors and missing fields before submission
- Flagging eligibility and authorization mismatches automatically
- Learning payer-specific denial patterns and applying them to future claims
- Reducing the manual review load on billing staff for routine claims
What AI does not eliminate
- Payer disputes that require human negotiation and clinical documentation
- Complex cases where diagnosis codes are genuinely ambiguous or contested
- Regulatory changes that the model has not yet been retrained on
- Errors introduced upstream in the intake or prescription process that lack sufficient data to detect
How Do You Build the Business Case for Upgrading Your DME Billing Software?
If you are a Director of Billing or a DME owner trying to justify a platform investment to leadership or to yourself, the business case comes down to a few numbers.
Start with your current denial rate and calculate what it costs you annually. Then estimate what a realistic reduction in that denial rate would be worth.
Add the cost of staff time spent on denial rework. If you have billing specialists spending a significant portion of their time on appeals and resubmissions, quantifying that time at fully loaded cost usually produces a compelling number.
Then weigh that against the platform cost, implementation time, and transition disruption. For most operations doing meaningful monthly billing volume, the math is not close. The question is usually which platform, not whether to upgrade.
What Questions Should You Ask a DME Billing Software Vendor Before Buying?
The right questions to ask a vendor depend on what you are trying to solve.
But there are several questions that apply regardless of your specific situation:
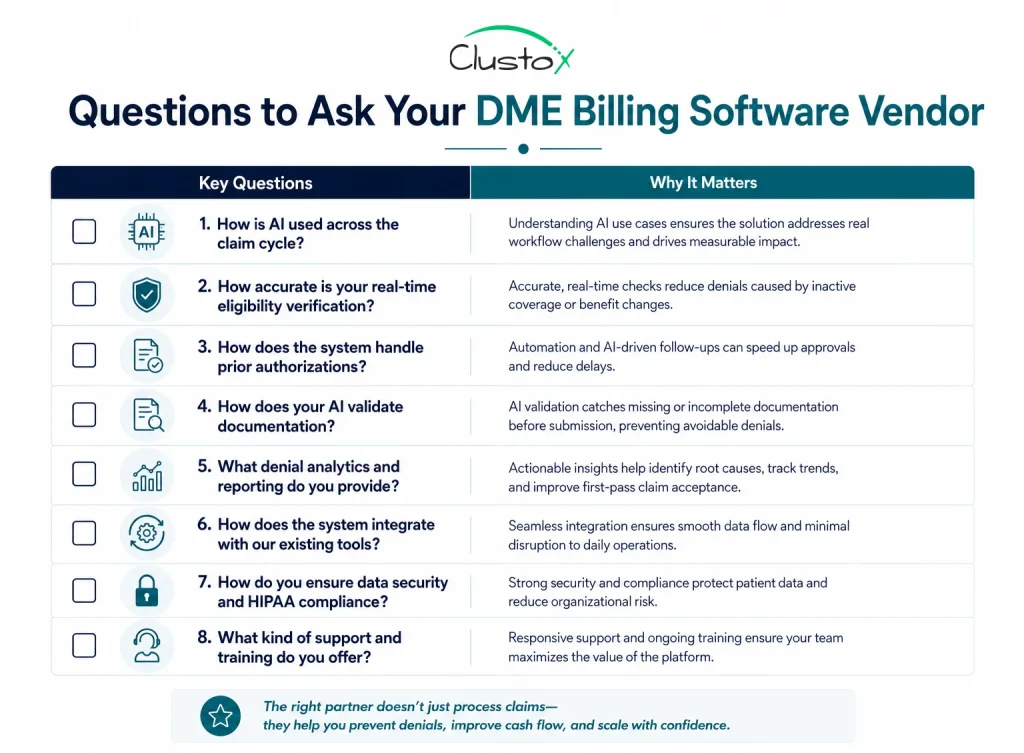
- Where exactly in the claim cycle does your AI intervene, and what does it flag?
- Does your eligibility verification run at intake only, or does it run again closer to delivery?
- How does your platform handle prior authorization tracking, including expiration monitoring?
- Can your documentation validation module check against payer-specific LCD requirements, not just generic CMS criteria?
- What does your denial analytics module feed back into the submission workflow?
- What integrations do you have with [your current platform, EHR, payer portals]?
- What does implementation look like, and what is a realistic timeline before you see error reduction?
- Can you provide case data from comparable DME operations showing actual denial rate changes?
Making the Move from Reactive to Preventive Billing
The difference between DME billing software that generates errors and software that prevents them is not a small one. It determines how much of your team’s week goes to denial work versus productive billing. It affects your cash flow, your headcount requirements, and the amount of revenue you recover versus write off.
In 2026, the tools exist to run a genuinely preventive billing operation. AI that monitors authorization status, verifies eligibility continuously, checks documentation against payer-specific requirements, and learns from your denial history is no longer an enterprise-only feature. It is available to practices of all sizes.
The question worth asking is not whether AI-powered DME billing software is worth exploring. It is whether the cost of not exploring it, measured in denied claims, rework hours, and recovered revenue, is something your operation can afford to keep absorbing.
If your current platform is letting errors through that a smarter system would catch, that is a solvable problem. The place to start is an honest look at your denial data.
Every denial your team touches is revenue your software failed to protect.
See how AI-powered DME billing software helps providers reduce preventable denials, accelerate reimbursements, and lower manual rework.
Frequently Asked Questions (FAQs)
Why do so many DME claims get denied?
Most DME claim denials trace back to a small set of root causes: missing or expired prior authorizations, inaccurate HCPCS codes or modifiers, stale eligibility data, and incomplete documentation. Standard billing software processes claims without verifying whether these inputs are correct. AI-powered platforms address this by checking for these issues automatically before submission.
Is AI billing software only for large DME providers?
No. While large operations were early adopters, cloud-based AI billing platforms have made these capabilities accessible to smaller and mid-size providers. Several platforms now offer AI-assisted features within standard subscription tiers. The business case for smaller operations is often just as strong, because denial rework absorbs a proportionally larger share of a small team's time.
Can AI replace DME billing specialists?
No. AI handles pattern recognition and pre-submission checks well. It does not handle payer negotiations, complex clinical documentation disputes, or the judgment calls that experienced billing specialists make on ambiguous cases. The practical outcome of AI adoption is that billing specialists spend less time on routine error correction and more time on high-value work that requires human judgment.
What is the difference between claim scrubbing and AI-powered billing?
Claim scrubbing applies a fixed set of rules to catch formatting and coding errors before submission. AI-powered billing goes further: it learns from denial patterns, cross-references payer-specific coverage criteria, monitors authorization status dynamically, and flags issues that rules-based scrubbers would miss. Scrubbing is a subset of what modern AI billing tools do.
How long does it take to implement AI DME billing software?
Implementation timelines depend on the platform and the complexity of your existing setup. A native AI feature activation within your current platform can happen in days. A full AI-native platform migration for a mid-size DME operation typically takes several weeks to a few months, including data migration, staff training, and payer enrollment updates. Ask your vendor for a specific implementation timeline based on your volume and system configuration.
Does AI billing software help with HIPAA compliance?
AI billing platforms that include audit logging, access controls, and documentation tracking can support your HIPAA compliance program. However, compliance obligations remain with your organization, not the software vendor. Review your business associate agreement with any platform you use and confirm what compliance features are included versus what requires additional configuration.
This article is intended for DME providers, operations leaders, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, accreditation standards) are accurate as of the review date; regulations change frequently, and providers should consult primary sources or qualified counsel for current requirements.