
If you run billing for a DME provider or you sign the P&L, there is a dollar amount sitting in your denial queue right now that your team will never recover. Not because the claims were invalid, but because the process of working denials is manual, slow, and consistently loses to payer timelines.
Industry discussions and provider benchmarks suggest DME denial rates often exceed 10%, particularly in documentation-heavy categories such as respiratory equipment and mobility devices. A substantial percentage of denied claims are recoverable when providers respond within appeal timelines and submit complete supporting documentation.
Most providers recover far less. The gap between what you could recover and what you actually recover is not a staffing problem. It is a systems problem.
Your billing team is spending hours each week manually reviewing payer response and remittance data, interpreting CARC and RARC codes, drafting appeal letters, and chasing documentation that should have been attached before the claim was submitted.
Denial management software is designed to close that gap. This article breaks down how modern denial management systems work, what the ROI looks like in DME-specific terms, and what a realistic 30/60/90-day implementation process looks like.
Why Do DME Providers Have Higher Denial Rates?
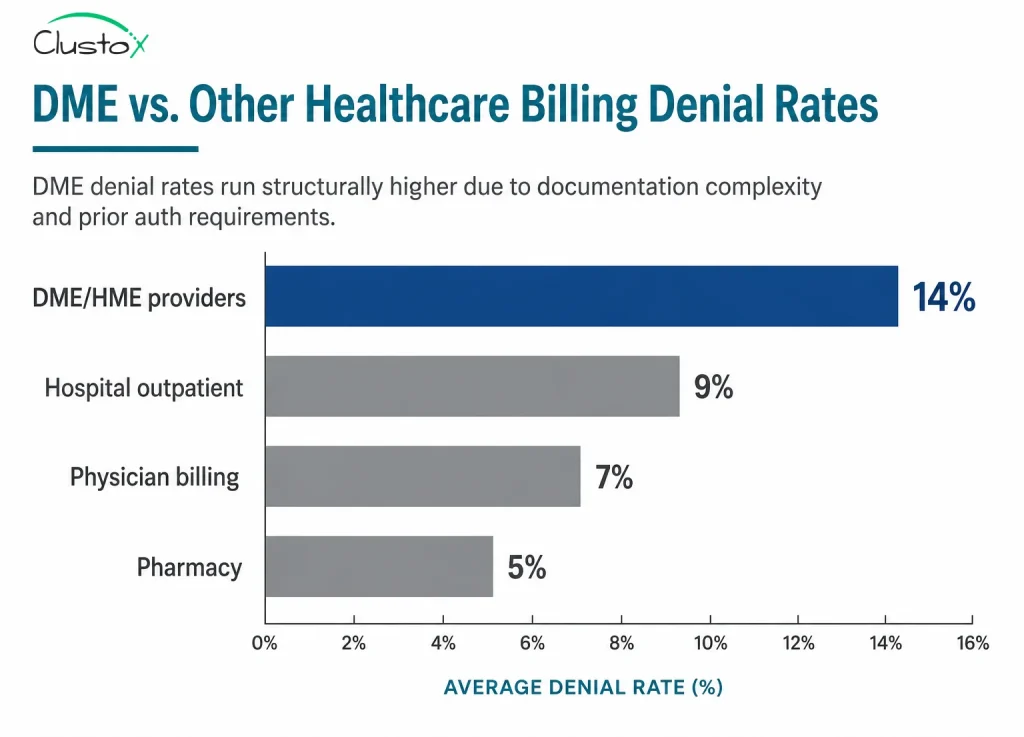
DME billing is structurally harder than most healthcare billing segments. You are navigating prior authorization requirements that vary by payer and product category, HCPCS code specificity that leaves little room for error, documentation requirements tied to clinical records you do not control, and Medicare competitive bidding rules that narrow your margin on every claim you collect.
According to AAHomecare, prior authorization and documentation issues are the leading drivers of DME denials, with medical necessity documentation and missing or incomplete records accounting for the majority of first-level rejections.
Table of Contents
Four structural reasons DME denial pain compounds
- Payer Variability: Medicare, Medicaid, and commercial payers each apply different coverage determination rules, appeal timelines, and documentation standards. A process that works for Medicare Advantage Plan A does not automatically work for Plan B.
- Short Appeal Windows: Medicare’s timely filing limit for redeterminations is 120 days from the date of the initial determination. Miss that window, and the claim is gone.
- Heavy Documentation Dependency: DME claims require physician orders, certificates of medical necessity (CMNs), and often detailed medical records. Gathering those documents after a denial is slower and more expensive than getting them right the first time.
- Volume: A mid-sized DME provider processing 5,000 claims per month at a 12% denial rate is working on 600 denied claims every 30 days, manually. That volume is where revenue leakage compounds. Your billing team triages; they work the obvious claims, and the marginal ones, recoverable but requiring 45 minutes of work each, pile up until they age out.
What Are the Types of DME Denials?
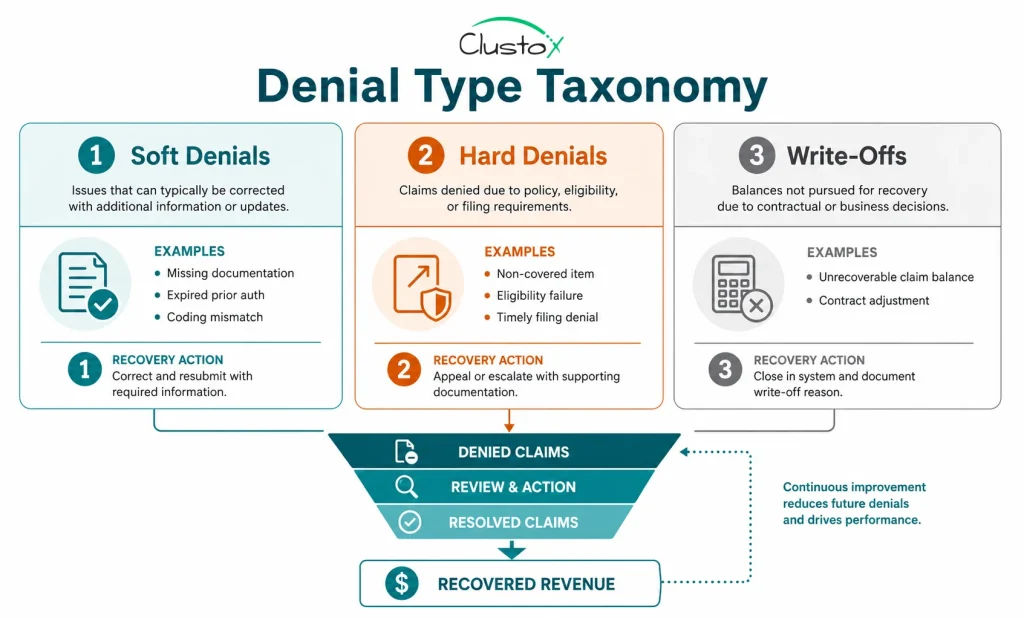
Before you can choose the right software or build the right process, you need to be precise about what kind of denials you are dealing with. The three categories have different recovery paths, different time horizons, and different automation profiles.
Soft Denials
A soft denial is a temporary, correctable rejection. The payer is not saying no to the claim; they are saying they cannot process it yet because something is missing or incorrect. Common soft denial types in DME include:
- Missing or expired prior authorization number
- Incorrect or mismatched modifier
- Missing physician signature on a CMN
- Eligibility not active on date of service
- Duplicate claim flag (often triggered by a resubmission error)
Soft denials are your highest-ROI recovery target. The fix is typically administrative: correct the error, attach the missing document, and resubmit. Denial management software is particularly effective here because the correction pattern is predictable. The same CARC code appears repeatedly for the same root cause, and the fix is the same each time.
Hard Denials
A hard denial is a final rejection where the payer has made a coverage or medical necessity determination. These require an appeal, not a correction and resubmission.
Hard denial types in DME include:
- Medical necessity not established
- Equipment not covered under the patient’s plan
- Benefit exhausted
- Non-covered diagnosis code
Hard denials require more work. You need a clinical rationale, supporting documentation, and a well-constructed appeal letter that addresses the specific denial reason. Automation helps here too, but it supports your billing staff rather than replacing their judgment.
Write-Offs
A write-off is a claim your organization has decided not to pursue further. Sometimes that decision is correct: the cost of appeal exceeds the expected recovery, or the appeal window has closed. But in most DME billing departments, write-offs also contain a significant number of claims that were workable but ran out of runway.
Industry estimates place the administrative cost of reworking denied claims anywhere from tens to more than one hundred dollars per claim depending on complexity and staffing structure.
For a $45 HCPCS item, the economics of manual rework do not hold up. Automation changes that equation by driving the per-claim rework cost down significantly.
Key Takeaway:
Your denial strategy needs different workflows for each category. Software that treats all denials the same is not denial management; it is a more organized version of the problem you already have.
How Much Revenue Are Unrecovered Denials Costing Your DME Practice?
Here is the math your CFO needs to see.
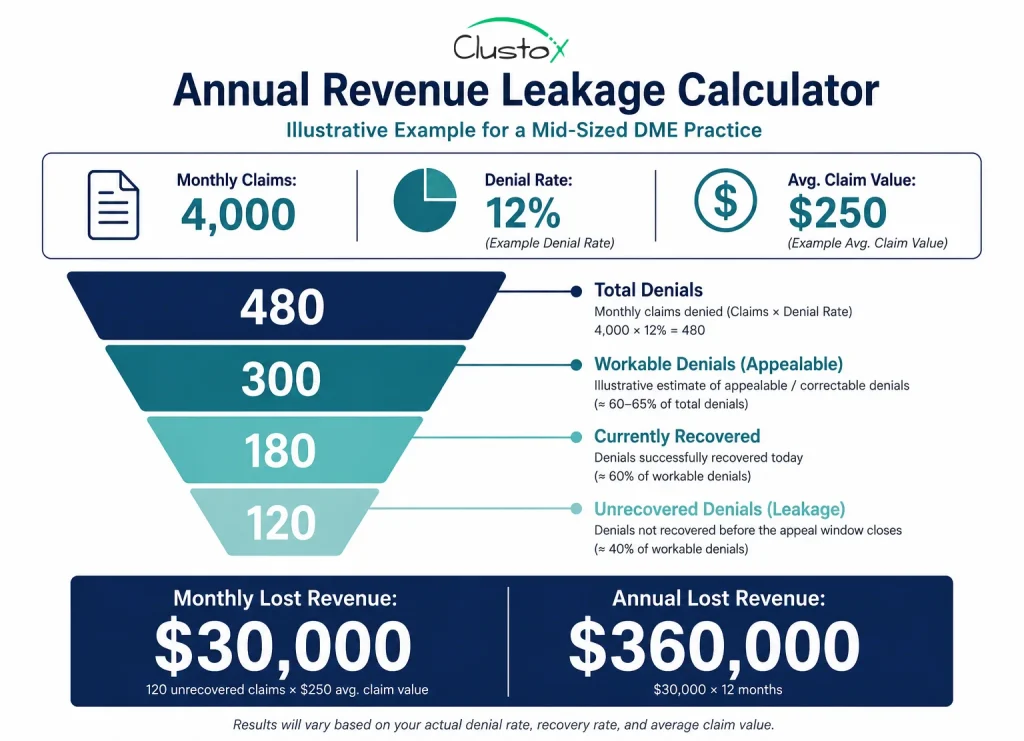
The following example illustrates how denial leakage compounds financially in a mid-sized DME operation
Assume your DME practice submits 4,000 claims per month. At a 12% denial rate, you have 480 denied claims per month.
Of those 480:
- Roughly 60–65% are soft denials or correctable hard denials, approximately 300 claims.
- Your team works on approximately 60% of workable denials before the appeal window closes; approximately 180 claims are recovered.
- That leaves 120 recoverable claims per month aging out without recovery.
For a larger provider processing 10,000 claims per month, the same ratios produce $900,000 in annual unrecovered revenue.
Those numbers do not include the staff cost of working the denials you do recover. If your billing team is spending 30 minutes per worked denial at a fully loaded labor cost of $35/hour, 180 monthly recoveries cost $3,150 in staff time, or $37,800 per year in recovery labor for revenue you should have captured on first submission.
The two-sided opportunity: recover more of the revenue you are currently writing off and reduce the labor cost of the revenue you do recover.
What Does Denial Management Software Actually Do?
Denial management software is a purpose-built layer in your revenue cycle that sits between your practice management system and your payer portals.
The core functions are:
| Function | What it does for your team |
|---|---|
| Denial ingestion & classification | Reads 277CA remittance files automatically, identifies denied claims, and classifies them by denial type using CARC and RARC code mapping, replacing manual remittance review. |
| Prioritization & work queue | Scores each denial by recoverable value, appeal deadline, and likelihood of recovery. Your team works on the highest-priority items first instead of triaging manually. |
| Appeal drafting | Generates a first-draft appeal letter using denial reason, patient record, and payer-specific template logic. Staff review and submit rather than write from scratch. |
| Root-cause tracking | Tags every denial to a root cause and surfaces patterns: 40% of denials flagged CARC 16. You have an upstream documentation problem. |
| Performance reporting | Denial rate by payer, by product category, first-pass resolution rate, appeal success rate, average days to resolution, live data, not a monthly spreadsheet. |
What it does not do
Denial management software does not replace your billing staff. It changes what they spend their time on. Instead of reading 277CA files manually and drafting appeals from scratch, they are reviewing auto-generated appeals, handling escalations, and working on upstream process changes that the root-cause data is pointing to.
How Does AI Classify DME Denials Automatically?
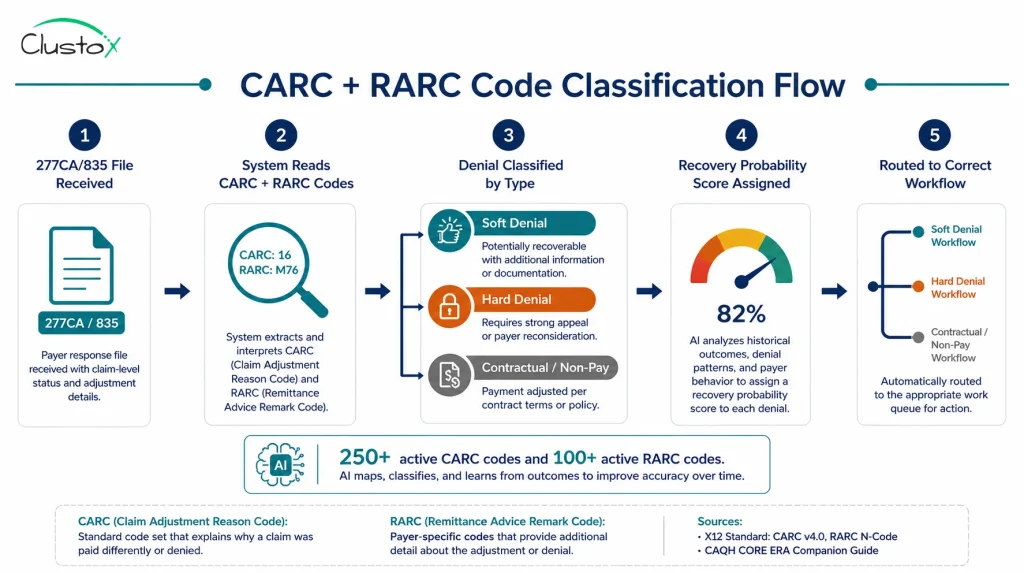
The 277CA is the HIPAA-standard transaction set that payers use to communicate claim status. It contains, at the claim and line-item level, the reason for any denial or adjustment.
Those reasons are encoded in two code sets:
- CARC (Claims Adjustment Reason Code): the primary reason for a claim adjustment. CARC 4 = contractual obligation. CARC 16 = claim lacks information. CARC 97 = payment included in the allowance for another service. There are over 250 active CARC codes.
- RARC (Remittance Advice Remark Code): supplemental information about the claim adjustment, adding specificity to the CARC reason. RARC M76 = missing or incomplete treatment authorization codes. RARC N479 = claim did not include patient’s reason for visit.
AI-augmented categorization applies a trained model to your incoming 277CA data to:
- Classify each denial by type (soft, hard, duplicate, contractual) using the CARC/RARC combination plus claim context.
- Match the denial to the most likely root cause from your provider’s historical pattern data.
- Assign a recovery probability score based on denial type, payer, product category, and your historical appeal success rate for similar denials.
- Route the denial to the appropriate workflow: auto-correct and resubmit, appeal draft queue, or escalation to a senior reviewer.
The accuracy of AI categorization improves over time as the model trains on your denial history. Models trained on larger historical denial datasets generally perform better because they can identify payer-specific denial patterns more consistently over time.
For your billing team, the practical impact is direct: instead of spending 20–30 minutes per denial reading remittance codes and deciding what to do, they spend two to three minutes reviewing an AI-generated classification and work recommendation, then executing.
How Fast Can Automation Draft a DME Appeal?
The appeal letter is where most DME billing departments lose the most time.
A well-constructed first-level Medicare redetermination request needs to:
- State the basis for the appeal clearly and specifically
- Reference the relevant coverage determination or Local Coverage Determination (LCD)
- Attach supporting documentation (physician order, CMN, medical records)
- Address the specific denial reason, not just restate that the equipment was medically necessary
- Be submitted within the payer’s appeal window
Doing this well takes an experienced biller 30–60 minutes per appeal depending on complexity. Appeal drafting automation generates a draft in minutes using the denial classification, patient claim history, payer-specific appeal templates, and LCD/NCD language where applicable.
Your biller reviews the draft, attaches any missing documentation, and submits. On straightforward soft denial corrections and common hard denial appeal types, the review and submission step takes 5–10 minutes rather than 45.
ONE LIMIT TO NAME DIRECTLY:Appeal automation does not improve the quality of your underlying documentation. If the physician’s CMN does not support medical necessity, no appeal letter will fix that. The software identifies those cases quickly, and that is valuable, but the resolution is upstream, not in the appeal.
How Is AI Changing the Way DME Providers Manage Denials?
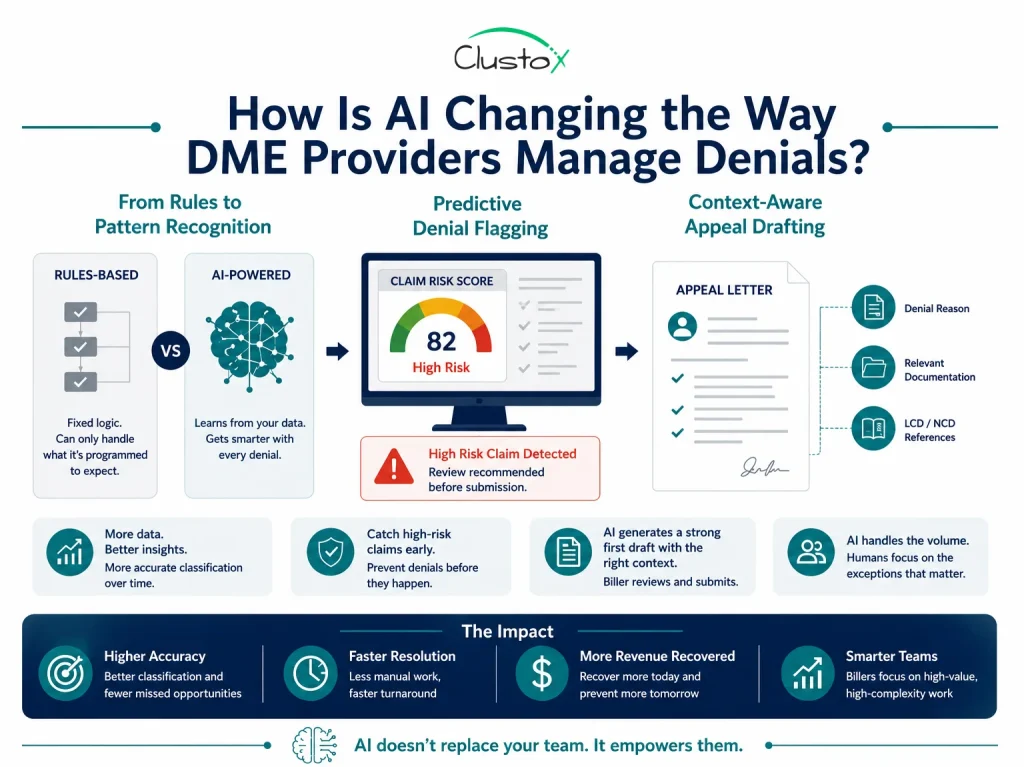
For most of its history, denial management ran on rules. If CARC code X appeared with payer Y, route to queue Z. Rules-based systems can only handle what they were programmed to expect, and DME denials rarely stay predictable for long.
AI changes the ceiling.
- From rules to pattern recognition: Where a rules-based system applies fixed logic, an AI-augmented system learns from your data. Every denial the software processes becomes a training signal. Over time the model builds a picture of your specific denial environment, which payers apply CARC 16 inconsistently, which product categories carry elevated hard denial risk, and which modifier combinations are triggering rejections before you have noticed the pattern.
- Predictive denial flagging: The most impactful AI implementations flag claims likely to be denied before they are submitted. The model scores each outgoing claim against your historical denial patterns and surfaces high-risk claims for a pre-submission review. A claim that would have been denied and worked for 45 minutes gets corrected in two minutes before it ever reaches the payer. This is where AI shifts denial management from a recovery function to a prevention function.
- Context-Aware Appeal Drafting: AI-augmented drafting generates context-aware appeal documents, not template letters. The system reads the specific denial reason, pulls relevant documentation, references the applicable LCD or NCD, and constructs an argument tailored to that payer’s known overturn criteria. Your biller reviews a document that is already 80% submission-ready.
How Do You Use Denial Data to Prevent Future Denials?
The most valuable long-term function of denial management software is not the appeals it generates. It is the upstream signal it produces.
Every denial your software classifies and resolves is data about a failure point in your revenue cycle.
Aggregate that data over 90 days and you will see patterns that are invisible when you are working denials one at a time:
- 28% of denials from Payer X are CARC 16 / RARC N290 (missing referral number): your intake team is not capturing referral numbers consistently for that payer’s plans.
- 19% of denials on CPAP supplies are CARC 18 (duplicate claim): your billing team is resubmitting without first verifying claim status, triggering duplicate flags.
- 22% of denials on power wheelchairs are CARC 50 (non-covered service): your front-end benefits verification is not checking wheelchair coverage before equipment is delivered.
Each pattern has a fix, a change to intake, to benefits verification, to claim scrubbing logic, or to how your team coordinates with referral sources. Denial management software surfaces those patterns. Your ops team resolves them.
Organizations that systematically use denial insights to improve intake, eligibility verification, and documentation workflows often reduce denial frequency over time.
The distinction matters for your CFO’s model: denial management software is not just a recovery tool. It is a revenue protection tool. The claims it helps you avoid denying in the first place are the highest-ROI outcome of the entire system.
Integration with Brightree, NikoHealth, and Claim Scrubbers
Here is the math your CFO needs to see.
The following example illustrates how denial leakage compounds financially in a mid-sized DME operation
Assume your DME practice submits 4,000 claims per month. At a 12% denial rate, you have 480 denied claims per month.
Of those 480:
- Roughly 60–65% are soft denials or correctable hard denials, approximately 300 claims.
- Your team works on approximately 60% of workable denials before the appeal window closes; approximately 180 claims are recovered.
- That leaves 120 recoverable claims per month aging out without recovery.
For a larger provider processing 10,000 claims per month, the same ratios produce $900,000 in annual unrecovered revenue.
Those numbers do not include the staff cost of working the denials you do recover. If your billing team is spending 30 minutes per worked denial at a fully loaded labor cost of $35/hour, 180 monthly recoveries cost $3,150 in staff time, or $37,800 per year in recovery labor for revenue you should have captured on first submission.
The two-sided opportunity: recover more of the revenue you are currently writing off and reduce the labor cost of the revenue you do recover.
What Does Denial Management Software Actually Do?

Denial management software is a purpose-built layer in your revenue cycle that sits between your practice management system and your payer portals.
The core functions are:
What it does not do
Denial management software does not replace your billing staff. It changes what they spend their time on. Instead of reading 277CA files manually and drafting appeals from scratch, they are reviewing auto-generated appeals, handling escalations, and working on upstream process changes that the root-cause data is pointing to.
How Does AI Classify DME Denials Automatically?
The 277CA is the HIPAA-standard transaction set that payers use to communicate claim status. It contains, at the claim and line-item level, the reason for any denial or adjustment.
Those reasons are encoded in two code sets:
- CARC (Claims Adjustment Reason Code): the primary reason for a claim adjustment. CARC 4 = contractual obligation. CARC 16 = claim lacks information. CARC 97 = payment included in the allowance for another service. There are over 250 active CARC codes.
- RARC (Remittance Advice Remark Code): supplemental information about the claim adjustment, adding specificity to the CARC reason. RARC M76 = missing or incomplete treatment authorization codes. RARC N479 = claim did not include patient’s reason for visit.
AI-augmented categorization applies a trained model to your incoming 277CA data to:
- Classify each denial by type (soft, hard, duplicate, contractual) using the CARC/RARC combination plus claim context.
- Match the denial to the most likely root cause from your provider’s historical pattern data.
- Assign a recovery probability score based on denial type, payer, product category, and your historical appeal success rate for similar denials.
- Route the denial to the appropriate workflow: auto-correct and resubmit, appeal draft queue, or escalation to a senior reviewer.
The accuracy of AI categorization improves over time as the model trains on your denial history. Models trained on larger historical denial datasets generally perform better because they can identify payer-specific denial patterns more consistently over time.
For your billing team, the practical impact is direct: instead of spending 20–30 minutes per denial reading remittance codes and deciding what to do, they spend two to three minutes reviewing an AI-generated classification and work recommendation, then executing.
How Fast Can Automation Draft a DME Appeal?

The appeal letter is where most DME billing departments lose the most time.
A well-constructed first-level Medicare redetermination request needs to:
- State the basis for the appeal clearly and specifically
- Reference the relevant coverage determination or Local Coverage Determination (LCD)
- Attach supporting documentation (physician order, CMN, medical records)
- Address the specific denial reason, not just restate that the equipment was medically necessary
- Be submitted within the payer’s appeal window
Doing this well takes an experienced biller 30–60 minutes per appeal depending on complexity. Appeal drafting automation generates a draft in minutes using the denial classification, patient claim history, payer-specific appeal templates, and LCD/NCD language where applicable.
Your biller reviews the draft, attaches any missing documentation, and submits. On straightforward soft denial corrections and common hard denial appeal types, the review and submission step takes 5–10 minutes rather than 45.
ONE LIMIT TO NAME DIRECTLY:Appeal automation does not improve the quality of your underlying documentation. If the physician’s CMN does not support medical necessity, no appeal letter will fix that. The software identifies those cases quickly, and that is valuable, but the resolution is upstream, not in the appeal.
How Is AI Changing the Way DME Providers Manage Denials?
For most of its history, denial management ran on rules. If CARC code X appeared with payer Y, route to queue Z. Rules-based systems can only handle what they were programmed to expect, and DME denials rarely stay predictable for long.
AI changes the ceiling.
From rules to pattern recognition
Where a rules-based system applies fixed logic, an AI-augmented system learns from your data. Every denial the software processes becomes a training signal. Over time the model builds a picture of your specific denial environment, which payers apply CARC 16 inconsistently, which product categories carry elevated hard denial risk, and which modifier combinations are triggering rejections before you have noticed the pattern.
Predictive denial flagging
The most impactful AI implementations flag claims likely to be denied before they are submitted. The model scores each outgoing claim against your historical denial patterns and surfaces high-risk claims for a pre-submission review. A claim that would have been denied and worked for 45 minutes gets corrected in two minutes before it ever reaches the payer. This is where AI shifts denial management from a recovery function to a prevention function.
Context-Aware Appeal Drafting
AI-augmented drafting generates context-aware appeal documents, not template letters. The system reads the specific denial reason, pulls relevant documentation, references the applicable LCD or NCD, and constructs an argument tailored to that payer’s known overturn criteria. Your biller reviews a document that is already 80% submission-ready.
How Do You Use Denial Data to Prevent Future Denials?
The most valuable long-term function of denial management software is not the appeals it generates. It is the upstream signal it produces.
Every denial your software classifies and resolves is data about a failure point in your revenue cycle.
Aggregate that data over 90 days and you will see patterns that are invisible when you are working denials one at a time:
28% of denials from Payer X are CARC 16 / RARC N290 (missing referral number): your intake team is not capturing referral numbers consistently for that payer’s plans.
19% of denials on CPAP supplies are CARC 18 (duplicate claim): your billing team is resubmitting without first verifying claim status, triggering duplicate flags.
22% of denials on power wheelchairs are CARC 50 (non-covered service): your front-end benefits verification is not checking wheelchair coverage before equipment is delivered.
Each pattern has a fix, a change to intake, to benefits verification, to claim scrubbing logic, or to how your team coordinates with referral sources. Denial management software surfaces those patterns. Your ops team resolves them.
Organizations that systematically use denial insights to improve intake, eligibility verification, and documentation workflows often reduce denial frequency over time.
The distinction matters for your CFO’s model: denial management software is not just a recovery tool. It is a revenue protection tool. The claims it helps you avoid denying in the first place are the highest-ROI outcome of the entire system.
Integration with Brightree, NikoHealth, and Claim Scrubbers
Denial management software delivers the most value when it integrates directly into the systems already managing claims, authorizations, and billing workflows. In DME environments, disconnected systems create duplicate work, slower appeals, and limited visibility into denial trends.
Brightree
Brightree is one of the most widely used DME practice management platforms. A denial management solution should integrate smoothly with Brightree workflows, including claims, authorizations, billing activity, and denial status tracking. The goal is to reduce manual handoffs while keeping billing teams inside familiar operational workflows.
NikoHealth
NikoHealth is designed for complex DME and HME operations, including respiratory and recurring supply workflows. Integration requirements are similar to Brightree: visibility into claim and authorization activity, denial tracking, workflow synchronization, and reporting alignment across systems. Denial insights should support existing operational workflows rather than forcing staff to manage work across disconnected platforms.
Claim scrubbers
Claim scrubbers operate upstream from denial management by identifying errors before claims are submitted to the payer. Common platforms used across healthcare revenue cycle operations include ClaimLogiq, Waystar, and Optum / Change Healthcare.
The most effective denial management workflows create a feedback loop between denials and claim scrubbing rules.
For example, if repeated CPAP denials are tied to incorrect modifier combinations or missing documentation, those patterns should become scrubber rules that prevent future claim errors before submission.
What to ask vendors about integration
- Request a live demonstration of the Brightree or NikoHealth integration, not static screenshots
- Ask how frequently data syncs between systems and whether any known data gaps exist
- Confirm whether updates are real-time or batch-based
- Ask how the platform handles denials that arrive through payer portals or outside standard ERA workflows
- Request references from DME providers using your specific PMS or billing platform
What Is the ROI on Denial Management Software?
The following example illustrates how improved denial recovery rates can translate into measurable financial impact for a mid-sized DME organization.
| Input / Assumption | Value |
|---|---|
| Monthly claim volume | 5,000 claims |
| Average allowed amount per claim | $275 [STAT NEEDED — CMS or AAHomecare] |
| Denial rate | 12% = 600 denied claims/month |
| Recoverable denials (soft + workable hard) | 60% = 360 claims |
| Current recovery rate (without software) | 55% of recoverable = 198 claims/month |
| Monthly unrecovered, recoverable revenue | 162 claims x $275 = $44,550 |
| Recovery rate with software | ~78% = 281 claims recovered/month |
| Additional monthly recoveries | 83 claims x $275 = $22,825 |
| Additional annual revenue recovered | $273,900 |
| Software cost (mid-tier) | $3,000/month = $36,000/year |
| Net annual benefit | $237,900 |
That does not include labor savings from reduced manual triage and appeal drafting (15–20 hours per week for a five-person billing team = $27,000–$36,000 annually at $35/hour fully loaded), denial rate reduction from root-cause prevention, or staff retention gains from more meaningful work.
What Does a Successful Denial Management Rollout Look Like?
A successful denial management rollout happens in phases, starting with baseline visibility, followed by workflow adoption, and then long-term optimization.
Here’s what a typical 30/60/90-day implementation timeline looks like for DME organizations.
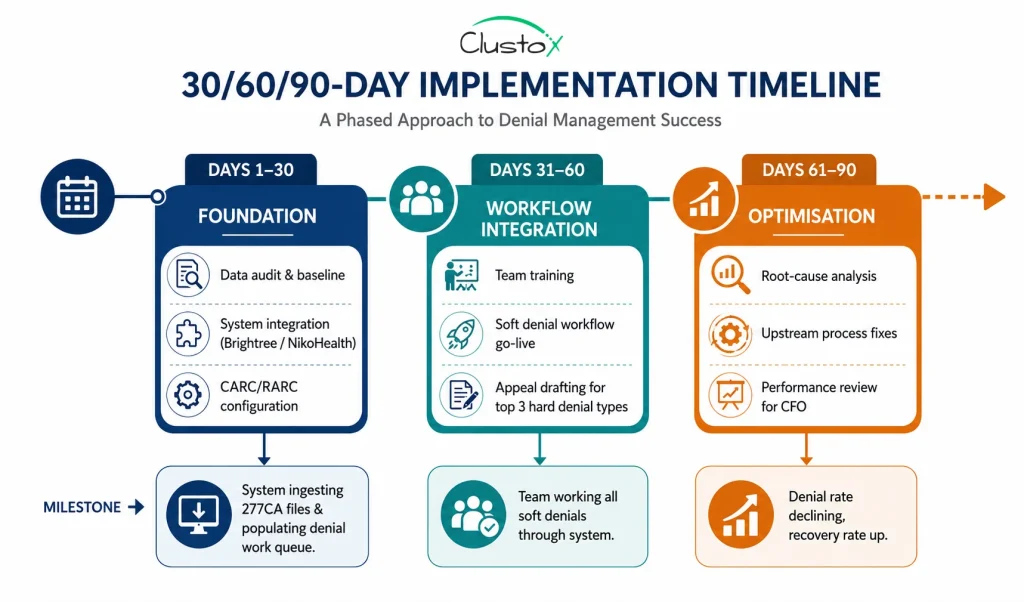
Days 1–30: Foundation
Before configuring the system, pull at least 90 days of historical denial data. Establish baseline metrics such as denial rate by payer, denial rate by product category, appeal success rate, and average days to resolution. If reporting is still handled manually through spreadsheets, consolidate and standardize the data first.
The goal during this phase is to build clean operational visibility before automation begins. Configure CARC/RARC mappings, validate payer response workflows, and complete integrations with billing or DME platforms such as Brightree or NikoHealth.
Days 31–60: Workflow integration
The billing team needs time to trust the workflow before adoption becomes consistent. During this phase, teams should work on live denials in the new system alongside their existing process, comparing system classifications against internal billing judgment. Disagreements are valuable because they often reveal configuration gaps, inconsistent workflows, or documentation issues.
Start with soft denials first before expanding into more complex appeal workflows. Track outcomes carefully: Was the denial categorized correctly? Was the appeal appropriate? Did the payer overturn the denial? Use those findings to refine configurations and improve workflow accuracy over time.
Days 61–90: Optimization and upstream prevention
By this stage, the system has accumulated enough denial data to identify recurring operational patterns. Run root-cause analysis reports to uncover the most common upstream failures, such as missing documentation, authorization gaps, or recurring payer-specific coding issues. Assign ownership and corrective action plans to each major issue.
Compare current denial and recovery metrics against the original baseline established during implementation. Use the findings to refine workflows, improve intake processes, and strengthen payer-specific documentation procedures. Present measurable operational improvements and recovery trends to leadership and finance stakeholders.
What Should You Look for When Buying Denial Management Software? (Buyer’s Checklist)
Use this when evaluating denial management software vendors. Organized by the questions that matter most for DME-specific implementations.
Integration
Does the vendor have a live, in-production integration with your PMS (Brightree, NikoHealth, TIMS)?
Is the integration API-based or file-based?
What is the claim data sync frequency?
Does the software write denial status and appeal outcomes back to your PMS?
How does it handle payer portal denials that do not arrive via 277CA?
Denial Classification
Does the software use CARC and RARC codes for classification, or proprietary reason codes?
Does it distinguish between soft denials, hard denials, and contractual adjustments automatically?
Can you see the classification logic (why did the system classify this denial this way)?
How does accuracy improve over time, and what is the training data based on?
Appeal Automation
Does the vendor have DME-specific appeal templates, or generic healthcare templates?
Do templates reference relevant LCDs and NCDs by product category?
Can your team customize templates without vendor involvement?
What is the vendor’s documented appeal overturn rate for DME clients? (Ask for references, not marketing claims.)
Root-Cause Analytics
Does the software produce root-cause reports by denial type, payer, and product category?
Can you set denial rate thresholds that trigger alerts?
Does the reporting environment connect to your claim scrubber?
Compliance and Security
Is the vendor HIPAA-compliant with a signed BAA?
Where is PHI stored, and what are the encryption standards?
What is the vendor’s uptime SLA and incident response protocol?
Commercial Terms
Is pricing per-claim, per-seat, or flat monthly?
Is there a minimum contract term? What are the exit terms?
What is included in the implementation fee?
Is ongoing CARC/RARC code maintenance included or a paid add-on?
Frequently Asked Questions
What is the average denial rate for DME providers?
There is no universally accepted benchmark for DME denial rates because performance varies by payer mix, equipment type, and workflow maturity. However, denials are widely recognized as a major operational challenge in DME billing due to documentation requirements, prior authorizations, and Medicare coverage rules.
What is a CARC code, and why does it matter for denial management?
A CARC (Claims Adjustment Reason Code) is the standardized code a payer uses to explain why a claim was adjusted or denied. There are 250+ active codes. Each one maps to a specific denial reason and determines the correct recovery path, correction and resubmit, appeal, or write-off. Denial management software reads CARC codes automatically and routes each denial accordingly.
How long does it take to implement denial management software?
Most DME providers with Brightree or NikoHealth integration are fully operational in 30–45 days. Integration and configuration take the first 30 days; team adoption and appeal workflow go-live happen in days 31–60; root-cause optimization closes out at 90 days.
What is the difference between denial management software and a claim scrubber?
A claim scrubber catches errors before a claim is submitted to the payer. Denial management software works after the payer has already denied the claim. The two systems are complementary, not interchangeable. The most effective DME revenue cycle stacks use a claim scrubber on the front end and denial management software to maximize recovery on the denials that get through.
What happens to denials that are genuinely not recoverable?
Denial management software should identify non-recoverable denials quickly, contractual adjustments, legitimate benefit exclusions, and timely filing misses and route them to write-off rather than consuming staff time on futile appeals. Accurately distinguishing recoverable from non-recoverable denials is one of the most valuable things the software does.
Does denial management software work for small DME providers?
It can, but the ROI math is tighter at lower claim volumes. The inflection point for most vendors is typically estimated to be 2,000–3,000 monthly claims. Below that volume, a claim scrubber investment may produce a higher ROI than a full denial management system.
How does AI improve denial categorization compared to rules-based systems?
AI improves denial categorization by identifying payer patterns, documentation issues, and recurring denial trends that static rules-based systems often miss. Unlike fixed rule engines, AI models can learn from historical denial data and adapt to evolving payer behavior over time.
Conclusion
Every DME billing department has two numbers that matter: the revenue it collects and the revenue it writes off. For most providers, that gap is not a staffing problem, it is a process problem. The manual denial workflow was not built for the volume, payer complexity, and documentation demands of modern DME billing. And it is costing you.
Denial management software does not patch that process. It replaces it. Claims that once aged out in a spreadsheet queue are classified, prioritized, and appealed in minutes. Root-cause patterns become upstream fixes that reduce your denial rate month over month.
The financial case is not subtle. A mid-sized DME provider can recover $200,000–$300,000 in annual write-offs at a software cost that is a fraction of that. Payback is measured in weeks.
The providers who move first build a revenue advantage that compounds. The ones who wait keep writing off claims they could have recovered.
Find the Revenue You’re Losing to Denials
Analyze your denial trends, recovery gaps, and preventable write-offs before they impact cash flow. Clustox helps DME providers automate denial workflows with AI-driven classification and appeal management.
⚠ DISCLAIMER
This article is intended for DME providers, operations leaders, billing directors, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, and accreditation standards) are accurate as of the review date; regulations change frequently, and providers should consult primary sources or qualified counsel for current requirements.