DME operators have been warned about the shift to AI-driven workflows for several years. The warnings were accurate, but the timeline was abstract. In 2026, it is no longer abstract.
The combination of forces bearing down on DME operations such as reimbursement compression, mandatory prior authorization expansion, intensified Medicare audit programs, and administrative wage inflation has moved healthcare workflow automation from a strategic option to an operational necessity.
This is not a technology argument. It is a cost-per-order argument. When CMS cuts reimbursement by 23% on high-volume HCPCS categories and your administrative cost per claim stays the same or rises, the math works against you on every order you process manually.
The operators who absorb that pressure without reducing margin are the ones who have removed manual touchpoints from their highest-volume workflows.
Not through headcount cuts, and not by working harder through Agentic AI services running on top of Brightree or NikoHealth that handle prior authorization, eligibility verification, denial management, and patient outreach without human input on routine cases.
This article makes the case for why automation is now a baseline requirement, not by describing what AI can do in theory but by showing the specific forces that have made manual workflows economically unsustainable, the workflows where automation is proven, the numbers those workflows are delivering, and what it takes to implement them without disrupting your operation.
What This Article Covers
- The six converging market forces that have made manual DME billing workflows economically unsustainable
- Why healthcare workflow automation is now a baseline operational requirement, not a competitive differentiator
- The specific workflows where automation is delivering measurable results in 2026
- What the transition from manual to automated operations actually looks like, step by step
- An honest account of the limits of what automation does not handle and where human oversight remains essential
- A pre-implementation readiness checklist for DME operators evaluating automation for the first time
The Six Forces Making Manual DME Billing Unsustainable
Manual billing workflows in DME were already under pressure before 2024. What changed is that multiple pressure sources converged simultaneously, eliminating the margin buffer that had kept manual operations viable for most providers.
Here are the 6 forces, with the data behind each one.
Table of Contents
Force 1: CMS Competitive Bidding Reimbursement Cuts
CMS Competitive Bidding Round 2024 cut reimbursement rates for high-volume HCPCS product categories by an average of 23%, according to AAHomecare’s 2024 Competitive Bidding analysis. For a provider billing $5M annually in affected categories, that is a $1.15M revenue reduction on the same order volume, with the same billing staff, and the same administrative cost structure.
When reimbursement per order falls, and administrative cost per order stays constant, the only way to maintain margin is to reduce the cost of processing each order. Manual workflows cannot do that. Automation can.
Force 2: Mandatory Prior Authorization Expansion
CMS expanded its Medicare Prior Authorization Program to cover five additional HCPCS categories in 2024, adding mandatory PA requirements for product categories that previously processed without them, according to CMS.gov.
Every new PA requirement adds an average of 6 to 9 days of processing time per complex order when handled manually, according to HFMA’s 2024 Revenue Cycle Benchmarking Report. For providers with high prior auth volume, this translates directly to deferred revenue, deferred patient care, and a billing team that cannot keep up.
Force 3: Intensified Medicare Audit Activity
TPE (Targeted Probe and Educate), RAC (Recovery Audit Contractor), ZPIC (Zone Program Integrity Contractor), and UPIC (Unified Program Integrity Contractor) audit programs are running simultaneously.
OIG’s 2023 DME billing compliance report found that improper payment rates for DME claims remained elevated, making DME providers a continued audit target. Each audit generates documentation requirements that consume billing team time that is not available when the same team is manually processing prior authorizations and chasing denied claims.
Force 4: Administrative Wage Inflation
Healthcare administrative wages increased 18 to 22% between 2021 and 2024, according to Bureau of Labor Statistics data. A billing team that cost $450,000 annually in 2021 costs $531,000 to $549,000 in 2024 for the same headcount.
That cost increase is entirely overhead; it does not produce more revenue unless the team is processing more orders. Manual workflows cap the orders a team can process. Automation removes that cap.
Force 5: The Soft Denial Write-Off Problem
The average DME provider writes off 6 to 12% of submitted claims as unrecoverable, per OIG’s 2023 DME billing compliance report. Most of those write-offs are soft denials: documentation gaps, prior authorization mismatches, HCPCS coding errors, and timely filing failures are all correctable on appeal if caught quickly and worked systematically.
A billing team already at capacity on manual prior auth processing does not have time to work a systematic denial appeal process. The soft denials become write-offs by default. Automation changes that equation.
Force 6: Patient Volume Growth Without Headcount Growth
DME demand is growing. The aging US population, expanded home health adoption post-pandemic, and increased CPAP and oxygen prescription rates are all increasing patient volume.
Providers are asked to do more, with the same team, at lower reimbursement per order. Manual billing workflows scale with headcount. Agentic AI workflows scale with compute, which means the marginal cost of processing an additional order approaches zero once the workflow is deployed.
Market Pressure Summary: Six Forces, One Direction
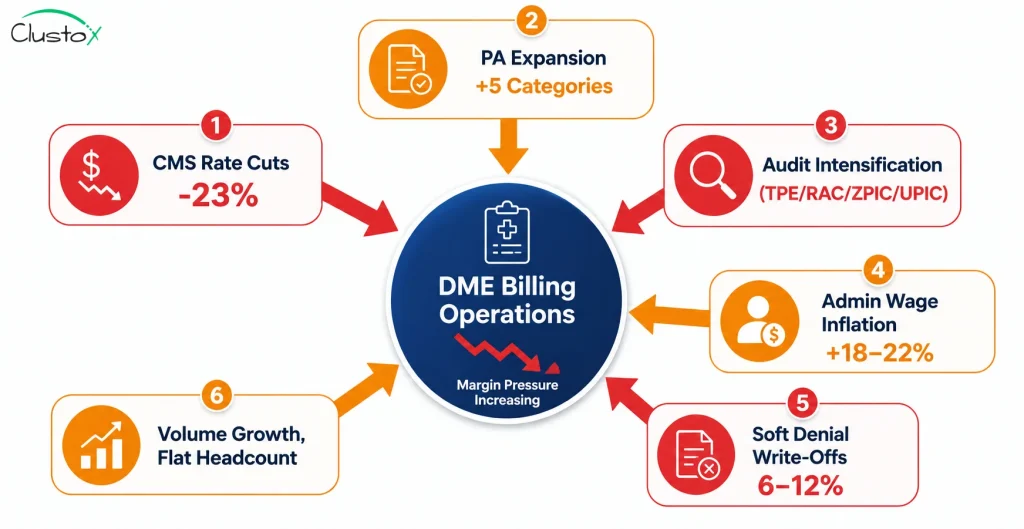
The table below summarizes all six forces, their quantified impact, and the operational consequence for DME providers still running manual workflows. Each row is a margin erosion event. Together, they represent a structural change in the economics of DME operations that manual workflows cannot absorb.
| Pressure Factor | Metric | Source | Operational Impact |
|---|---|---|---|
| CMS Competitive Bidding 2024 | 23% avg reimbursement cut on high-volume HCPCS categories | AAHomecare, 2024 | Every order earns less admin cost per order; becomes critical |
| CMS Prior Authorization Expansion | 5 new HCPCS categories added to mandatory PA program | CMS.gov, 2024 | More orders require PA manual processing time multiplies |
| Medicare Audit Intensification | TPE, RAC, ZPIC, UPIC all active simultaneously | OIG.hhs.gov, 2024 | Documentation burden increases; audit exposure rises |
| Staffing Cost Inflation | Healthcare admin wages up 18–22% since 2021 | BLS, 2024 | Manual processing costs more while reimbursement falls |
| Soft Denial Write-Off Rate | 6–12% of submitted DME claims written off as unrecoverable | OIG, 2023 | Revenue lost to preventable, automatable errors |
| Prior Auth Cycle Time | 6–9 days average per complex order (manual) | HFMA, 2024 | Delayed revenue, deferred patient care, staff bottleneck |
Why Is Healthcare Workflow Automation Now an Operational Baseline?
For most of the last decade, DME providers who automated billing workflows had a competitive advantage. They processed more orders, recovered more denials, and maintained lower administrative cost per claim than their manual-workflow competitors.
That advantage was real, and it was optional. A provider who chose not to automate could remain viable by running a disciplined manual operation.
That is no longer true. The six forces above have collectively moved the breakeven point. A provider running a well-managed manual billing operation today, with a competent team, low error rate, and good payer relationships, is still absorbing a structural margin penalty that compounds with every order processed. The penalty is not a function of management quality.
It is a function of the unit economics: lower reimbursement per order times constant administrative cost per order equals a margin problem that no amount of manual efficiency recovers.
Healthcare workflow automation changes the denominator. When prior authorization is handled by an Agentic AI agent on Brightree or NikoHealth, the cost per PA submission does not scale with claim volume; it scales with compute, which is orders of magnitude cheaper than billing labor.
When eligibility verification runs automatically at three points in the order lifecycle, the eligibility-driven denial rate drops without adding a single staff hour. When denial management runs on a continuous AI classification-and-appeal cycle, the 6 to 12% write-off rate becomes an 18 to 27% recovery rate. None of these outcomes require hiring. They require deploying the right workflow on top of a platform your team already uses.
The Workflows Where Automation Is Delivering Results
Not every DME workflow benefits equally from automation in 2026. The six below are where the evidence is strongest; each has a measurable before-and-after outcome, a defined implementation path, and a production track record on Brightree and NikoHealth.
1. Prior Authorization: From 6+ Days to Under 48 Hours
An Agentic AI prior authorization workflow pulls the order and Letter of Medical Necessity from Brightree or NikoHealth, verifies documentation completeness against CMS coverage criteria and payer-specific PA requirements, submits via the payer portal or fax API, and monitors for status, escalating only genuine exceptions to a human reviewer. For standard HCPCS categories including E0601 (CPAP devices) and E1390 (oxygen concentrators), turnaround drops from 6 to 9 days to under 48 hours. The same billing team handles two to three times the prior auth volume.
2. Eligibility Verification: Stopping Denials Before They Happen
Healthcare providers are increasingly using AI Agent Services to run real-time 270/271 checks at three points: intake, PA submission, and claim drop. They flag benefit-limit proximity and coordination-of-benefits issues before the claim goes out. Eligibility-driven soft denials drop 15 to 22% with multi-point verification, per Clustox implementation data. The denial management workload drops correspondingly because fewer claims need to be worked after the fact.
3. Denial Management: Recovering Revenue That Was Being Written Off
AI denial management classifies every incoming denial by root cause (documentation gap, authorization mismatch, HCPCS modifier error, or timely filing), drafts the appropriate appeal with supporting documentation, and submits it within the payer’s window automatically. It also feeds denial patterns back upstream to prevent the same error on future claims. DMEs implementing this workflow recover 18 to 27% of previously written-off soft denials within 90 days of deployment, per Clustox implementation data and OIG 2023 benchmarks.
4. Patient Intake and Qualification: Cutting Per-Patient Admin Time by 80%
AI intake agents pull referral orders, verify insurance via real-time eligibility, confirm qualification criteria against CMS coverage requirements, and pre-populate the order record in Brightree or NikoHealth. The billing coordinator reviews a completed intake record rather than building one from scratch. Staff time per new patient intake drops from 45 to 60 minutes to 8 to 12 minutes for standard cases, an 80% reduction in per-patient admin time.
5. CPAP Re-Supply Outreach: Capturing Revenue That Was Being Left Behind
AI voice agents and SMS agents contact CPAP patients on their preferred channel at the appropriate re-supply interval, confirm supply needs, capture refusals or deferrals, and push confirmed orders back into Brightree or NikoHealth for fulfillment. Phone reach rates improve from 30 to 40% (phone-only) to 65 to 75% (voice plus SMS), and monthly re-supply order capture improves 30 to 40%, according to Clustox implementation data.
6. Oxygen Recertification: Eliminating Missed Certification Windows
Automated recertification workflows track every active oxygen patient’s recertification schedule, send alerts to referring physicians 30 and 14 days before deadlines, collect updated clinical documentation, and flag at-risk patients for human escalation. Near-zero missed recertifications are achievable with a properly configured workflow. The audit exposure from lapsed certifications drops accordingly.
What DME Operators Are Seeing: Results Across Six Workflows
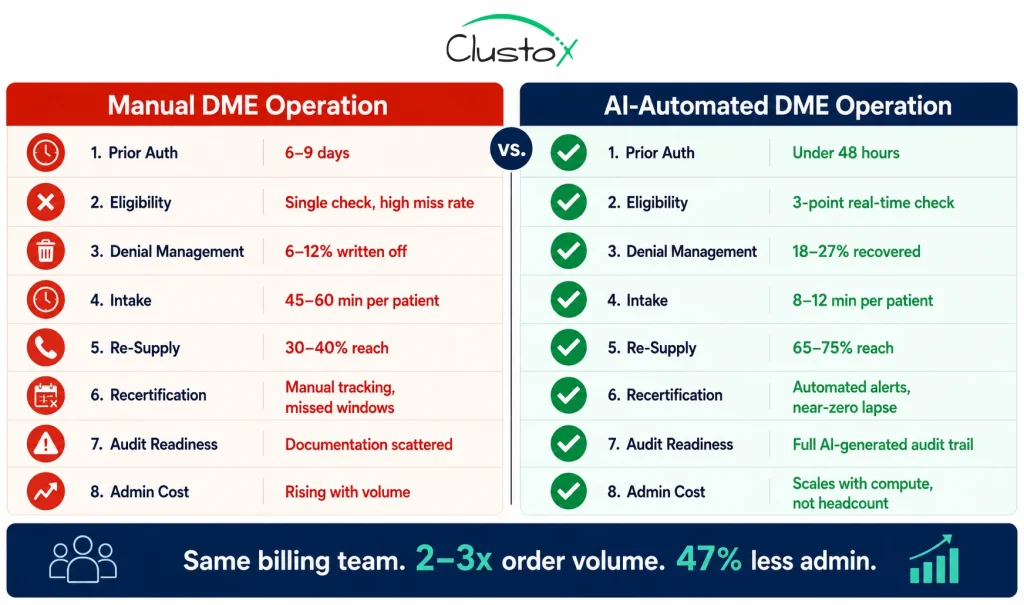
The table below reflects Clustox implementation data across DME clients on Brightree and NikoHealth, validated against HFMA 2024, AAHomecare 2024, and OIG 2023 benchmarks. Results vary by payer mix, order volume, and existing workflow maturity.
| Workflow | Before → After | Operational Outcome |
|---|---|---|
| Prior Authorization | 6–9 days → under 48 hours | Billing team handles 2–3x volume. Same headcount. Revenue recognized faster. |
| Eligibility Verification | Single intake check → 3-point check | Eligibility-driven soft denials drop 15–22%. Fewer claim reworks. |
| Denial Management | 6–12% write-off → 18–27% recovered | Soft denials that were written off become recovered revenue within 90 days. |
| Patient Intake | 45–60 min → 8–12 min per patient | Intake staff freed for exception review and patient escalation. |
| CPAP Re-Supply Outreach | 30–40% phone reach → 65–75% reach | 30–40% more re-supply orders per month from the same patient base. |
| Oxygen Recertification | Manual tracking → automated alerts | Near-zero missed certifications. Audit exposure significantly reduced. |
| Overall Admin Overhead | Baseline → 47% reduction | Same team. More throughput. Lower cost per order. Sustainable margin. |
How the Transition From Manual to Automated Actually Works
The most common mistake DME operators make when approaching automation is treating it as an all-or-nothing switch. It is not. The implementations that succeed follow a defined sequence: audit the current state, build the first workflow, prove the model, then expand. Here is what that sequence looks like in practice.

Step 1: The AI Readiness Audit (48 Hours)
Before any workflow is built, a 48-hour AI Readiness Audit maps your current state: which workflows are consuming the most billing team time, which payers represent the highest PA and denial burden, what your API access situation is on Brightree or NikoHealth, and what data quality issues exist in your current platform. The output is a prioritized workflow plan with a fixed-cost ROI model. This step takes two days and prevents six months of implementation regret.
Step 2: Prior Authorization First
Every successful DME automation starts with prior authorization. It is the highest-volume, highest-friction workflow and the one where AI performance is most immediately measurable. The prior authorization agent is deployed and run in parallel with the manual workflow for two to four weeks to validate accuracy, then cut over as the primary submission path. Most operations reach 85-plus percent automation of routine PAs within 30 days of go-live.
Step 3: Eligibility Verification, Second
Once prior auth is stable, eligibility verification is added. Multi-point eligibility checks at intake, PA submission, and claim drop prevent the downstream denial rate from accumulating. The billing team begins seeing the downstream effect: fewer soft denials reaching the denial management queue because fewer claims are going out with eligibility errors.
Step 4: Denial Management Third
With prior auth and eligibility automated, the denial management workflow becomes more surgical: fewer incoming denials overall, and the ones that do arrive are classified and appealed automatically. The billing team’s workload on denial management shifts from manually working every denial to reviewing AI-drafted appeals before submission, a review process that takes minutes, not hours, per claim.
Step 5: Intake, Re-Supply, and Recertification
Patient intake automation, CPAP re-supply voice and SMS outreach, and oxygen recertification tracking are added in Months 4 through 6 once the billing-side workflows are stable. These workflows address the revenue leakage that occurs outside the claim cycle: patients who never complete intake, CPAP patients who do not reorder, and oxygen patients whose recertification lapses without the provider knowing.
What Are the Current Limitations of Healthcare Workflow Automation for DME Providers?
Healthcare workflow automation in DME is delivering the results described above. It is not a complete solution without limits. Operators who understand these limits design better implementations. Those who ignore them get expensive surprises.
1. Non-Standard Payer Portal Interfaces
AI agents work most reliably on payer portals with consistent, well-documented interfaces. Some regional Medicare Advantage plans and Medicaid managed care organizations use non-standard portals that require a manual fallback path until the portal interface is mapped. Expect 10 to 20% of your payer mix to require manual fallback at initial deployment, declining as the agent learns each portal over time.
2. LMN Quality from Referring Physicians
An AI documentation check confirms whether a Letter of Medical Necessity contains the required elements for the ordered HCPCS category. It cannot fix a clinically inadequate LMN. Providers with weak referral relationships will see elevated PA denial rates regardless of automation quality. Automation amplifies the quality of your documentation inputs; it does not substitute for them.
3. Complex Rehab Technology Categories
For CRT product categories, including custom power wheelchairs (K0800–K0899), complex seating, and custom orthotics, documentation requirements are individualized and payer-specific.
AI assists with documentation completeness and submission logistics, but the clinical coverage determination still requires a trained specialist in the loop. Do not attempt to fully automate CRT prior authorization without human clinical review.
4. Medicare Audit Response Decisions
AI can assemble documentation packages for TPE, RAC, ZPIC, and UPIC audit responses, organizing claim records, pulling supporting documentation, and formatting the package according to audit contractor requirements.
The substantive response decision requires human review and, in material cases, qualified healthcare counsel. Automate the assembly. Keep the decision human.
5. Legacy Multi-System Environments
Providers running TIMS alongside secondary billing systems and spreadsheet workflows have significantly higher integration complexity than those on a single modern platform.
If you are in this environment, the most cost-effective path is usually platform consolidation before AI implementation, not simultaneously with it. A TIMS-to-NikoHealth migration followed by AI deployment typically takes less total time than attempting both in parallel.
Pre-Implementation Readiness Checklist
Before any vendor conversation or implementation commitment, verify the following. These are
| Readiness Check | What to Verify |
|---|---|
| API access confirmed | Verify your DME platform (Brightree or NikoHealth) provides API access at the level needed for prior auth, eligibility, and claims. If you're on TIMS or a legacy system, assess integration feasibility before committing to an AI timeline. |
| HIPAA BAA in place | Confirm your AI infrastructure provider (AWS Bedrock, Azure OpenAI, GCP Vertex AI) can sign a HIPAA Business Associate Agreement. All PHI processing must occur within a BAA-eligible environment. Non-negotiable. |
| Payer priority list defined | Identify your top 10 payers by claim volume. Confirm which ones the automation vendor fully supports and which require manual fallback. Get this in writing. |
| Data quality reviewed | Pull a sample of your last 90 days of orders and claims. Identify missing fields, incomplete patient records, and coding inconsistencies. Clean data is what makes automation accurate. |
| Denial root cause analysis done | Pull your last 6 months of denied claims. Classify by denial type: documentation, authorization, eligibility, coding, timely filing. This tells you which automation workflow to build first. |
| Billing team briefed | The billing team's role changes post-automation. Communicate what changes before go-live. Identify your exception review leads the people who will own the AI's flagged cases. |
| Baseline metrics documented | Record your current prior auth cycle time, eligibility denial rate, write-off percentage, and orders per billing FTE. You cannot measure a 47% improvement without a baseline. |
| Vendor ROI methodology confirmed | Ask every vendor: how will you measure what we achieved? If they cannot answer, they are not measuring outcomes. Walk away. |
 .
.
Not Sure Where to Start? That Is Exactly What We Map For You
We identify which workflows are costing you the most, which automation delivers the fastest ROI, and what your implementation roadmap looks like at a fixed price, with no obligation to proceed.
Frequently Asked Questions
Which DME workflow should I automate first?
Prior authorization, without exception. It is the highest-volume manual workflow, the one with the longest cycle time (6 to 9 days per complex order), and the one where AI performance is most immediately measurable. Once prior auth automation is stable, eligibility verification is the natural second step because it prevents the downstream denial rate from accumulating. Denial management, patient intake, CPAP re-supply, and oxygen recertification follow in that order for most operations.
How does healthcare workflow automation work with Brightree or NikoHealth?
Agentic AI workflows integrate with Brightree or NikoHealth via API. They read order data, patient records, and claim information from the core platform, execute the automated workflow (prior auth submission, eligibility check, denial appeal), and write results back into the platform. Brightree API access is available through its integration framework. NikoHealth provides modern REST API access that makes integration faster and less expensive. Legacy platforms such as TIMS have limited API surfaces that significantly increase integration complexity.
How quickly will I see ROI from healthcare workflow automation?
Most operations see measurable ROI within the first billing cycle after the prior authorization and eligibility workflows go live, typically 30 to 60 days. Denial recovery ROI is visible within 90 days of the denial management workflow deployment, as previously written-off denials begin returning as recovered revenue. Full ROI across all six workflows is typically realized within 6 months of complete deployment, based on Clustox implementation data.
Is Agentic AI for DME workflows HIPAA compliant?
It can be, but HIPAA compliance in AI workflows requires deliberate architecture. All AI processing of Protected Health Information must occur under a signed HIPAA Business Associate Agreement with the infrastructure provider. AWS Bedrock, Azure OpenAI Service, and GCP Vertex AI are all BAA-eligible. Compliance is not a feature of the AI model; it is an infrastructure and architecture requirement. HHS guidance on BAA requirements is available at HHS.gov.
What happens to billing staff when workflows are automated?
Billing staff shift from order processors to exception reviewers. Instead of manually building every prior authorization submission, they review the 10 to 15% of cases the AI flags as requiring human judgment, such as peer-to-peer escalations, documentation gaps, and non-standard payer responses. This is a meaningful shift in the daily role, and it requires clear communication and training before go-live. Operations that handle this transition well typically report improved staff satisfaction, because coordinators spend more time on judgment-based work and less on repetitive data entry.
What is the cost of not automating DME workflows?
The cost is quantifiable: the margin penalty of processing each order at a higher administrative cost than your reimbursement can sustain. A provider billing 500 complex orders per month with an administrative cost of $40 per order and a 23% reimbursement cut is absorbing $460,000 in annualised margin erosion that does not recover through manual efficiency gains. That number grows with volume. The cost of not automating compounds every billing cycle.
Can DME automation handle Medicare Advantage prior authorization requirements?
For the major Medicare Advantage plans, including UnitedHealthcare, Humana, CVS/Aetna, and Elevance, yes, with well-established integration paths. For smaller regional MA plans with non-standard portal interfaces, expect a manual fallback path at initial deployment. Most vendors can confirm specific payer coverage before implementation. Get the payer support list in writing and confirm which payers are fully automated versus requiring fallback; this is one of the most important vendor evaluation questions.
How long does DME workflow automation take to implement?
A 48-hour AI Readiness Audit identifies priorities and confirms feasibility before any implementation begins. The prior authorization workflow typically reaches go-live 8 to 12 weeks from the signed contract, assuming API access is confirmed, and the readiness audit is complete. Adding eligibility verification adds 3 to 4 weeks. Denial management adds 4 to 6 weeks. Full multi-workflow deployment covering all six workflows typically takes 4 to 6 months. Legacy platform environments add 4 to 8 weeks to all timelines.
What is the difference between rules-based automation and Agentic AI in DME workflows?
Rules-based automation executes a fixed sequence of steps based on predefined conditions; if X, then Y. It handles predictable, structured workflows but cannot adapt to non-standard responses or navigate payer portals that behave differently across sessions. Agentic AI is goal-directed: it can navigate payer portals, handle exceptions, draft appeals, and manage multi-step processes that require conditional judgment, all without human input on routine cases. The difference in outcomes is significant: rules-based tools typically automate 40 to 60% of prior auth submissions; Agentic AI workflows consistently automate 85-plus percent within 90 days of deployment.
Conclusion
The question for DME operators in 2026 is not whether to automate healthcare billing workflows. The six forces described in this article, including reimbursement cuts, PA expansion, audit intensification, wage inflation, denial write-offs, and volume growth without headcount growth, have answered that question. The question is which workflow- not through headcount cuts, and not by working to automate first- and how to do it without disrupting the operation in the process.
The answer to the first question is consistent across operations of different sizes and payer mixes: prior authorization first, eligibility second, denial management third.
The answer to the second question is a phased implementation that starts with a two-day readiness audit, proves the prior auth model within 30 days of go-live, then expands systematically through the remaining workflows over four to six months.
The operators who start this process now will be processing two to three times the order volume with the same billing team by the end of 2026. The operators who wait will be processing the same volume at a higher cost per order, against lower reimbursement, with a billing team that has less time to recover the denials that are quietly eroding their margin every month.
The 47% administrative reduction is not a projection. It is what happens when the manual touchpoints are removed from the 6 workflows described in this article. The technology is proven. The implementation path is defined.
Modern healthcare workflow automation combines AI and ML Services with intelligent workflow orchestration to reduce administrative overhead, accelerate revenue cycles, and improve operational scalability. What varies is when you decide to start.