Automated insurance verification is transforming how DME companies handle patient eligibility checks. Instead of manually logging into multiple payer portals, running eligibility checks one patient at a time, and re-entering data into platforms like Brightree or NikoHealth, modern verification systems automate the entire workflow in real time.
Using HIPAA 270/271 transactions and direct payer API integrations, these systems can verify coverage, retrieve detailed benefit information, identify authorization requirements, and update order management systems in under 60 seconds. The result is faster patient onboarding, fewer eligibility-related claim denials, reduced administrative workload, and a more efficient intake process for DME providers operating at scale.
As referral volumes increase and Medicare Advantage plans become more complex, manual verification workflows are becoming harder to sustain. Automated eligibility verification helps DME providers improve operational efficiency, reduce costly billing errors, and accelerate order confirmation for patients who need equipment without delays.
In this guide, you’ll learn how automated insurance verification works for DME companies, how it integrates with platforms like Brightree and NikoHealth, which vendors lead the market, what implementation requires, and how to evaluate the right solution for your organization.
What This Article Covers
- Why manual insurance verification fails DME providers operationally and financially
- How automated eligibility verification works, including real-time API and 270/271 query methods
- Integration requirements for Brightree, NikoHealth, and TIMS
- A vendor comparison across the most common DME eligibility tools
- Performance benchmarks and real numbers from DME operations running automation
- Where automated verification falls short and how to plan for it
- A practical 8-point buyer’s checklist for evaluating vendors
- 10 frequently asked questions from DME operators and billing directors
Why Does Manual Insurance Verification Cost DME Providers So Much?
Manual insurance verification creates operational bottlenecks for DME providers in three major areas: staff productivity, claim denials, and delayed patient order confirmation. As referral volumes grow and payer requirements become more complex, these inefficiencies compound quickly.
A typical manual eligibility check requires intake coordinators to log into multiple payer portals, enter patient demographics, navigate plan-specific benefit screens, verify coverage details, and then manually re-enter that information into systems like Brightree or NikoHealth. For patients with secondary or tertiary insurance coverage, the process often needs to be repeated multiple times.
While a single verification may only take 12 to 20 minutes, the operational impact becomes significant at scale. A DME team processing 50 to 150 referrals per week can spend dozens of staff hours every week on eligibility checks alone instead of focusing on patient communication, intake completion, or authorization follow-ups.
Table of Contents
The financial impact is even larger when verification errors reach billing. Manual workflows increase the risk of transposed member IDs, incorrect benefit interpretation, missed authorization requirements, and incomplete documentation. These small intake errors often become costly downstream denials.
According to the Change Healthcare Denial Reason Report (2023), eligibility and benefit verification issues account for approximately 23.9% of all initial claim denials in healthcare, making them one of the most common and most preventable denial categories.
The recovery process is equally expensive. The AAPC Coding and Billing Benchmarks Report (2023) found that up to 75% of denied claims are recoverable, but recovering them requires additional staff time, appeals workflows, resubmissions, and payer follow-up that many DME billing teams struggle to manage efficiently at scale.
For Medicare-focused DME suppliers, the compliance risk is even more serious. CMS Medicare FFS Improper Payment Data (2023) reported improper payment rates exceeding 25% in certain competitive bidding categories, with documentation and eligibility-related issues cited as major contributing factors.
In practice, manual verification does not just slow operations down — it increases administrative costs, creates avoidable denial risk, delays patient onboarding, and limits how efficiently DME providers can scale their intake teams.
Manual insurance verification costs DME providers in three ways that compound each other: staff time per transaction, claim denials from verification errors, and patient attrition from delayed order confirmation.
A typical manual eligibility check requires a coordinator to log into the correct payer portal, enter patient demographics, navigate benefit screens that vary by plan, note the relevant coverage details, then re-enter that information into Brightree, NikoHealth, or whatever order management system the provider uses.
For a multi-insurance patient, that process runs twice or more. Across a team handling 50 to 150 referrals per week, the accumulated hours are significant.
The accuracy problem is equally damaging. Manual data entry from payer portals introduces transposition errors, benefit misreads, and overlooked authorization requirements. When those errors reach the billing stage, they generate preventable denials that require appeals, write-offs, or resubmissions.
How Does Automated Insurance Verification Work for DME Companies?
Automated insurance verification for DME replaces manual portal checks with real-time system-to-system queries. The process is faster, more thorough, and produces structured data that feeds directly into your order workflow without a coordinator re-entering anything.
There are 2 primary query methods:
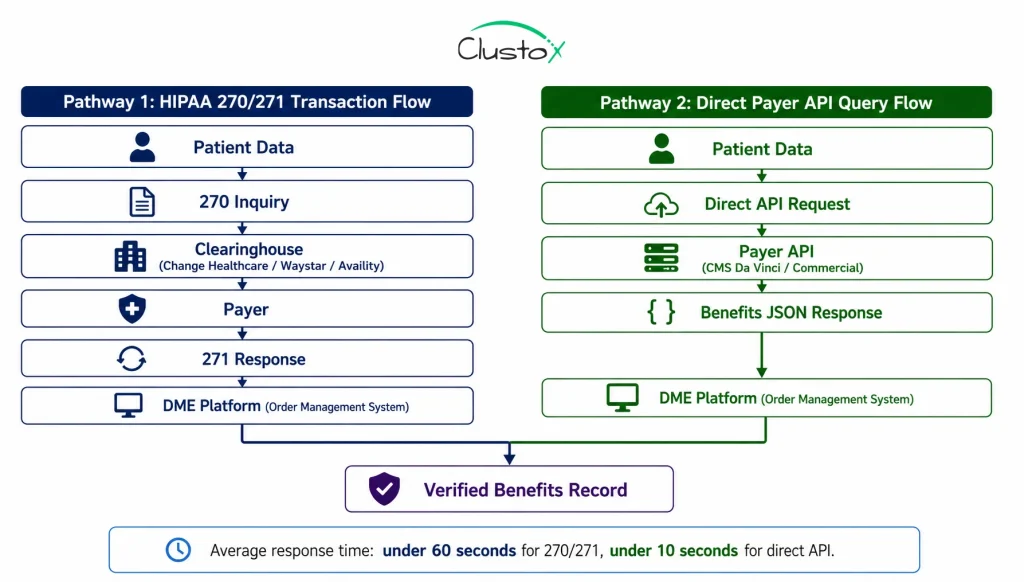
1. HIPAA 270/271 Eligibility Transactions
The HIPAA 270 transaction is an electronic eligibility inquiry: the system sends a structured request to the payer containing the patient’s insurance ID, date of birth, and the requested service type. The payer responds with a 271 transaction that includes benefit details, coverage status, deductible balances, co-pay amounts, and authorization requirements.
This method works with most major payers, including traditional Medicare, Medicare Advantage plans that process 270/271, and the majority of large commercial carriers. Clearinghouses such as Change Healthcare, Waystar, and Availity act as intermediaries, routing queries to hundreds of payers through a single connection.
2. Direct Payer API Connections
An increasing number of payers, including CMS for Medicare Advantage under the CMS interoperability mandates, now offer direct API connections for eligibility verification. Direct API queries return richer benefit detail than 270/271 in many cases, including DME-specific benefit tiers, formulary coverage, and prior authorization flags.
CMS’s Da Vinci PDex implementation guide, adopted by major Medicare Advantage plans under the CMS Interoperability and Prior Authorization Final Rule, is expanding real-time eligibility data access significantly in 2024 and 2025.
What are the Benefits Detail Returned by Automated Verification?
A well-configured automated verification system returns more than a simple active/inactive status. For DME operations, the relevant benefit data includes:
- Coverage active or inactive, with effective and termination dates
- DME benefit tier and any applicable co-insurance or co-pay amounts
- Deductible balance remaining for the benefit period
- Out-of-pocket maximum status
- Whether prior authorization is required for the specific HCPCS code
- Secondary and tertiary insurance details, where available
- Medicare Advantage plan formulary tier for the requested equipment
How Does Automated Eligibility Verification Integrate With Brightree and NikoHealth?
Integration depth varies significantly between eligibility vendors and DME platforms. This is the most important evaluation dimension for any DME operator, because a system that verifies eligibility accurately but still requires a coordinator to re-enter that data into Brightree has not solved the problem.
1. Brightree Integration
Brightree supports eligibility verification through its native connection to a limited set of clearing houses and through the Brightree API for third-party integrations. The native Brightree eligibility check returns basic coverage status. Third-party systems that integrate via the Brightree API can write richer benefit data, authorization flags, and secondary insurance details directly into the patient and order record.
API access requires a formal request to Brightree support and may carry additional costs depending on your contract tier.
2. NikoHealth Integration
NikoHealth’s API-first architecture makes integration with automated eligibility systems more straightforward than Brightree in most cases. Eligibility verification results, including detailed benefit breakdowns and authorization flags, can be written directly into the patient intake record via NikoHealth’s API without additional configuration overhead.
3. TIMS and Legacy Platform Integration
TIMS and Universal Software Solutions have older API infrastructure. Third-party eligibility automation vendors typically handle these platforms via an RPA (robotic process automation) layer that reads and writes to the system’s interface rather than through a direct API call. This approach works but introduces additional dependencies that require monitoring and occasional intervention.
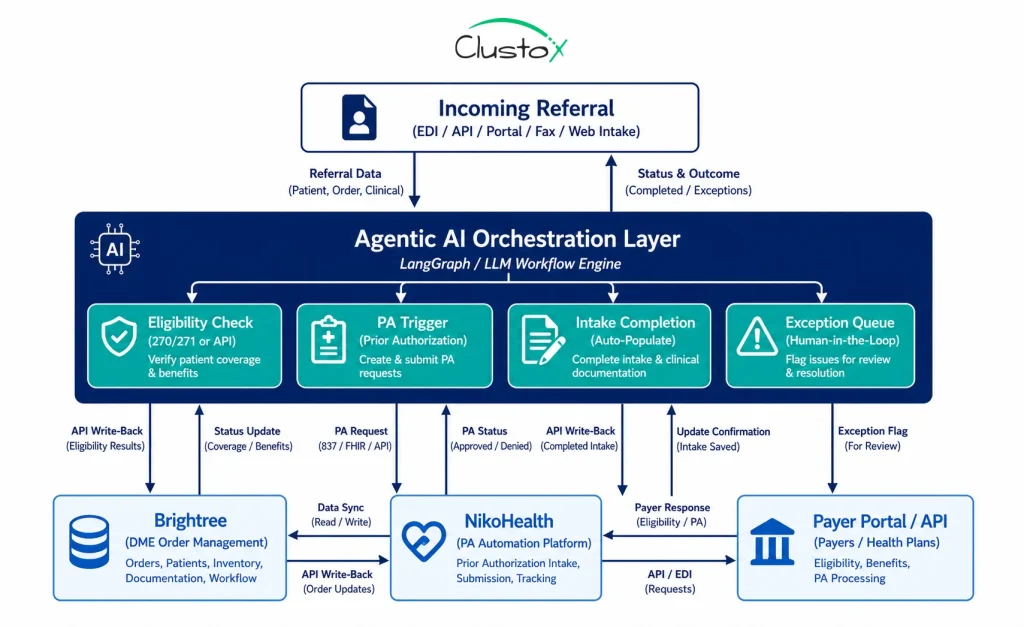
4. The Agentic AI Layer
A more recent integration pattern uses an Agentic AI orchestration layer, built on frameworks like LangGraph or LLM-based workflow engines, that sits above both the eligibility verification tool and the DME platform.
This layer handles the logic of when to run verification, how to interpret ambiguous results, when to flag for human review, and how to trigger downstream steps (prior authorization, intake completion, order creation) based on verification outcomes. For high-volume DME operations processing 200 or more referrals per month, this orchestration layer is what transforms isolated eligibility checks into a continuous, automated intake workflow.
Under the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), payers are required to support electronic prior authorization and interoperable eligibility data access, with compliance deadlines beginning in 2026 for most Medicare Advantage and Medicaid managed care plans. Source: CMS Interoperability and Prior Authorization Final Rule (2024)
How Does Automated Verification Compare to Manual Checks in Practice?
The operational difference between manual and automated insurance verification is not marginal. It changes what a coordinator’s day looks like, what your denial rate looks like, and how quickly patients get confirmed for equipment.
| Metric | Manual Verification | Automated Verification |
|---|---|---|
| Eligibility check speed | 1 to 3 days (manual portal) | Under 60 seconds (real-time API) |
| Payers checked simultaneously | 1 at a time | Primary + secondary + tertiary |
| Accuracy on first submission | 60% to 70% clean | 85% to 92% clean |
| Staff time per verification | 12:20 minutes | Under 2 minutes (exception review only) |
| Medicare Advantage handling | Manual plan lookup required | Automated benefit layer detection |
| Integration with Brightree | Manual re-entry required | API write-back, no re-entry |
| Audit documentation | Inconsistent, coordinator-dependent | Timestamped log per transaction |
DME providers who implemented real-time eligibility automation reported an average 18% reduction in eligibility-related claim denials within six months, according to a 2023 survey by the Healthcare Financial Management Association (HFMA). Source: HFMA Revenue Cycle Automation Survey (2023)
The staff time difference is particularly significant at scale. A coordinator running 40 manual eligibility checks per day at 15 minutes each spends 10 hours on verification alone. The same coordinator reviewing exceptions from an automated system that handles 95% of checks automatically spends under 2 hours, with the remaining time available for document follow-up, patient communication, and complex case handling.
What Does Implementation Require for DME Operators?
Most DME providers can implement automated insurance verification in 3 to 6 weeks if the prerequisites below are in place. The narrower timeline compared to full intake automation reflects the fact that eligibility verification is a discrete, well-defined workflow with established transaction standards.
1. Technical Prerequisites
Active enrollment for HIPAA 270/271 eligibility transactions through your clearinghouse (Change Healthcare, Waystar, Availity, or equivalent).Most mid-size and larger DME providers already have this in place.
Brightree, NikoHealth, or TIMS with API access enabled or confirmed for the integration method the vendor uses.
A payer ID list for your top 20 to 30 payers, including Medicare, Medicare Advantage plan IDs, Medicaid MCO identifiers, and commercial payer IDs.This is required to configure query routing.
A HIPAA-compliant data environment with a signed Business Associate Agreement with any new vendor in the data path.
2. Operational Prerequisites
A documented payer matrix showing which payers require prior authorization for which HCPCS codes.Eligibility verification systems use this to surface authorization flags accurately.
A defined exception workflow: who handles verifications that return inactive coverage, insufficient benefits, or error codes, and what the escalation path looks like.
A named implementation lead who owns the integration can access your DME platform’s API settings and serves as the primary contact during testing.
3. Implementation Timeline
- Weeks 1 to 2: Clearinghouse connectivity confirmed, payer IDs loaded, and test transactions run against the sandbox environment.
- Weeks 2 to 3: Integration with Brightree or NikoHealth configured, and write-back fields mapped to the correct record locations.
- Weeks 3 to 4: Parallel run (automated verification alongside existing manual process) to validate accuracy before full cutover.
- Weeks 4 to 6: Full production deployment with exception monitoring and coordinator training on the new exception queue workflow.
Which Vendors Handle Automated Insurance Verification for DME?
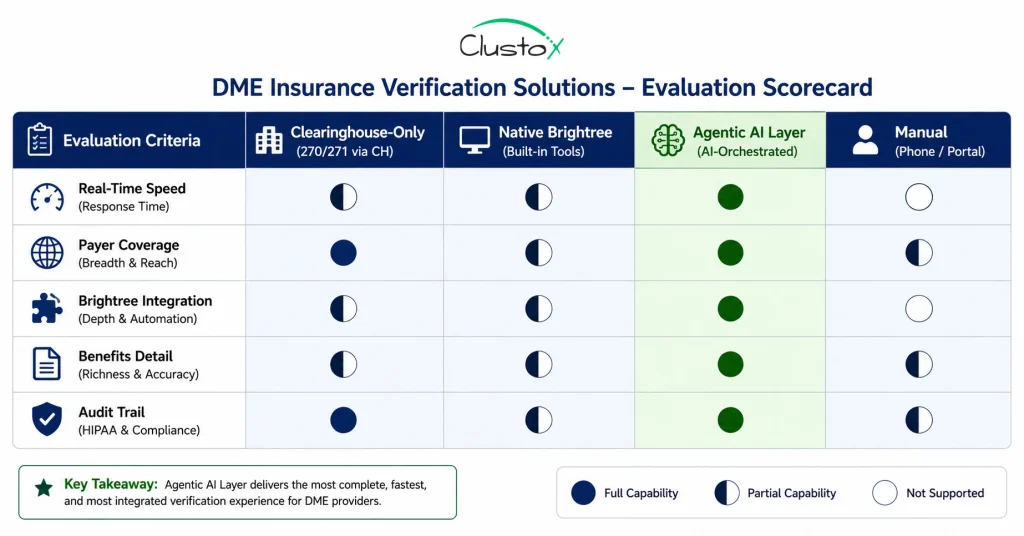
The eligibility verification market for DME has a few well-established clearinghouse-based tools and an emerging category of Agentic AI-based solutions that layer on top of clearinghouse connectivity to add DME-specific logic.
Here is a comparison of the most relevant options:
| Solution | Query Method | Real-Time | DME Integration | Pricing Model |
|---|---|---|---|---|
| Waystar / Zirmed | 270/271 + direct payer | Yes | Yes (Brightree) | $0.15:to:$0.45/check |
| Change Healthcare | 270/271 + direct payer | Yes | Yes (most DME sys) | $0.12:to:$0.40/check |
| Availity | 270/271 | Yes | Limited | Free portal; API extra |
| Agentic AI layer (e.g. Clustox) | API + 270/271 + payer portal | Yes + benefit detail | Native Brightree + NikoHealth | Per-referral or SaaS tier |
| Brightree native check | 270/271 only | Basic | Native | Included in Brightree contract |
For DME providers running Brightree or NikoHealth at volume, the most important distinction is not which clearinghouse the vendor uses, as most route through the same networks, but whether the system integrates deeply enough with your DME platform to eliminate re-entry and whether it surfaces DME-specific benefit details (authorization flags, benefit tier, HCPCS-level coverage) rather than just active/inactive status.
What Real Numbers Are DME Providers Seeing From Verification Automation?
Performance data from DME operations running automated eligibility verification shows consistent improvements across the metrics that matter most to operations and billing leadership. The numbers below reflect what is achievable with a well-configured integration; individual results vary by payer mix, referral volume, and the extent to which exception-handling workflows are optimized.
- Eligibility-related denial rate: 18 to 25% reduction within 6 months of implementation, primarily from eliminating data entry errors and benefit misreads.
- Staff time per eligibility check: from 12 to 20 minutes (manual) to under 2 minutes (exception review only), representing a 6-10x throughput improvement per coordinator FTE.
- First-pass clean claim rate: improvement from a 60-70% baseline to 82-90%, driven by accurate benefit data at the point of order creation.
- Order confirmation speed: same-day confirmation for clean referrals versus 1-3 day delays with manual verification.
- Coordinator capacity redeployment: coordinators who previously ran 40 to 60 manual checks per day now handle 150 to 200 referrals per day, with automation managing routine checks.
A 2022 CAQH Index report found that fully electronic eligibility and benefit verification saves an average of $2.07 per transaction compared to manual processing, translating to over $9 billion annually in potential healthcare industry savings. Source: CAQH Index 2022: Closing the Gap
For a DME provider processing 300 referrals per month, reducing coordinator time per eligibility check from 15 minutes to 2 minutes recovers approximately 65 staff hours per month. At a fully loaded hourly rate of $28 to $35 for an intake coordinator, that is $1,820 to $2,275 in recovered capacity per month from eligibility automation alone, before factoring in denial reduction.
Where Does Automated Insurance Verification Fall Short?
Automated eligibility verification solves a well-defined problem effectively. It has clear limits that operators need to understand before assuming the technology will handle all cases without exception.
1. Payer Portal Coverage Gaps
Not every payer supports 270/271 transactions or direct API queries. Some smaller Medicaid managed care organizations, regional commercial plans, and Medicare Advantage plans with proprietary portal requirements cannot be queried electronically. For these payers, manual checks remain necessary. Ask any vendor for their specific payer coverage list, not a headline number.
2. Benefits Data Accuracy Variation
270/271 responses reflect the payer’s benefits data as of the query date. That data can lag behind actual plan changes, particularly mid-year benefit modifications or coordination-of-benefits updates. An automated system that returns a clean eligibility result does not guarantee the claim will pay; it confirms the benefit structure as the payer’s system currently represents it.
3. Medicare Advantage Plan Complexity
Medicare Advantage plans set their own formularies, DME benefit tiers, and prior authorization requirements, and these vary significantly across plans even within the same parent carrier. An eligibility check that confirms MA coverage is active does not automatically confirm that the specific HCPCS code is covered at the expected benefit level. DME-specific benefit tier verification requires either a direct payer API with plan-level formulary access or a separate manual check for MA beneficiaries.
4. Coordination of Benefits Edge Cases
Patients with multiple active insurance policies present ongoing challenges. Automated systems check primary and secondary insurance when both ID numbers are provided, but they do not reliably detect duplicate coverage, policy terminations that have not yet propagated through the payer’s system, or coordination-of-benefits arrangements that exist outside the payer’s eligibility data. These cases remain coordinator-dependent.
5. HCPCS-Level Authorization Flags
Generic eligibility verification confirms that a patient has DME coverage. It does not always confirm whether the specific HCPCS code being requested is covered under that patient’s plan, whether there are quantity limits, or whether a rental-versus-purchase determination affects authorization. Systems with HCPCS-level benefit lookup address this, but not all eligibility vendors offer it. Verify explicitly whether your vendor’s system returns HCPCS-specific authorization and coverage information.
Buyer’s Checklist: How Should DME Operators Evaluate Verification Software?
Use these eight criteria when evaluating automated insurance verification vendors. The goal is to find a system that integrates deeply with your DME platform, covers your actual payer mix, and produces the benefit detail your team needs to create clean orders, not just a system that checks a box on a feature list.
| Criterion | What to Evaluate |
|---|---|
| Real-Time Eligibility API | Does the system query payers in real time via 270/271 or direct payer API? Batch processing delays defeat the purpose. Confirm response time SLAs. |
| Payer Network Coverage | How many payers are supported for real-time queries? Ask for the specific payer list, not a percentage. Confirm Medicare, Medicare Advantage, Medicaid, and your top 10 commercial payers. |
| Benefits Detail Depth | Does verification return just active/inactive status, or does it return co-pay, deductible, out-of-pocket maximum, DME-specific benefit tier, and authorization requirements? Shallow checks still cause downstream errors. |
| Secondary Insurance Handling | Can the system verify primary and secondary simultaneously? Coordination of benefits errors are a major source of DME claim denials. |
| Brightree / NikoHealth Write-Back | Does verified eligibility data write directly into the patient record in your DME platform, or does a coordinator still need to re-enter it? Write-back eliminates the last manual step. |
| HIPAA-Compliant Architecture | Does the vendor provide a signed BAA? Is PHI encrypted in transit (TLS 1.2+) and at rest (AES-256)? Request their most recent SOC 2 Type II report. |
| Exception Workflow | What happens when eligibility returns inactive, insufficient benefits, or an error? Is there a structured coordinator queue, or does the exception just stall? |
| Audit Trail and Logging | Does every eligibility transaction generate a timestamped, immutable log? This is required for ACHC and BOC accreditation compliance and for TPE and RAC audit defense. |
Frequently Asked Questions
How fast is real-time eligibility verification compared to manual checks?
A real-time eligibility query via HIPAA 270/271 typically returns a response in under 60 seconds. Direct payer API connections often return responses in under 10 seconds. By comparison, a manual eligibility check through a payer portal typically takes 12 to 20 minutes per patient when you account for login, navigation, data review, and re-entry into the DME system. For a team running 50 referrals per week, that is 10 to 17 hours of staff time that automation reduces to exception-handling only.
Does Automated Eligibility Verification Work With Medicare And Medicare Advantage?
Traditional Medicare (fee-for-service) is fully supported via HIPAA 270/271 transactions and the Medicare Beneficiary Identifier (MBI). Medicare Advantage plans are more variable: most major carriers (UnitedHealthcare, Humana, Aetna, and Cigna) support electronic eligibility queries, but benefit detail depth varies by plan. The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) is expanding electronic eligibility access for Medicare Advantage plans through 2026. Confirm your specific MA plan list with any vendor before assuming full coverage.
What is a HIPAA 270/271 transaction?
A HIPAA 270 transaction is an electronic eligibility inquiry that a healthcare provider sends to a payer (or through a clearinghouse) to verify a patient's insurance coverage. The payer responds with a HIPAA 271 transaction that includes coverage status, benefit details, deductible information, and authorization requirements. These transactions are standardized under HIPAA Electronic Data Interchange (EDI) rules, which means they follow a consistent format across payers, allowing a single clearinghouse connection to reach hundreds of payers. Most DME providers already have clearinghouse relationships that support 270/271; automated eligibility systems plug into that existing infrastructure.
Will automated eligibility verification integrate with our Brightree system?
Most automated eligibility verification vendors support Brightree integration through the Brightree API, allowing verified benefit data to write directly into the patient record and order shell without coordinator re-entry. The depth of that integration varies: some vendors write only coverage status, while others write full benefit details including co-pay, deductible balance, authorization flags, and secondary insurance. Brightree API access may require a formal support request to Brightree and could incur additional contract costs. Confirm API access availability and fees with Brightree before committing to a vendor that depends on it.
What does DME eligibility verification actually check for?
A thorough automated eligibility check for DME returns: coverage active/inactive status with effective and termination dates; DME benefit tier and applicable co-pay or co-insurance amounts; deductible balance for the current benefit period; out-of-pocket maximum status; whether prior authorization is required for the relevant HCPCS code; secondary and tertiary insurance details where available; and Medicare Advantage plan-specific formulary tier information where the payer supports it. Basic clearinghouse checks return the first two items. Systems with DME-specific logic and direct payer API connections return the full list, which is what is needed to create a clean order without downstream billing errors.
How does verification automation reduce DME claim denials?
Eligibility and benefit verification errors account for approximately 23.9% of initial claim denials in healthcare, making them one of the most preventable denial categories. Automated verification reduces denials by eliminating the data entry errors that occur when coordinators manually read and re-enter benefit information, by surfacing authorization flags at the point of order creation rather than at billing, and by checking secondary insurance simultaneously with primary coverage to prevent coordination-of-benefits errors from reaching the claims stage. DME providers running automated verification typically report eligibility-related denial rate reductions of 18:to:25% within the first six months.
Is automated insurance verification HIPAA-compliant?
Automated eligibility verification systems transmit Protected Health Information (PHI) as part of every query. Compliance depends on the vendor's technical controls and your contractual agreements, not the software category itself. Any vendor in the data path must sign a Business Associate Agreement (BAA), operate under HIPAA Security Rule (45 CFR Part 164) technical safeguards (encryption in transit and at rest, access controls, audit logging), and maintain documented breach notification procedures. Review current HIPAA Security Rule guidance at HHS.gov. Request the vendor's most recent SOC 2 Type II report as part of your evaluation.
What happens when an eligibility check returns inactive coverage or insufficient benefits?
A properly designed automated verification system routes exception cases to a structured coordinator queue with a summary of what the check returned and what needs to happen next. Exception types include: coverage inactive (coordinator verifies with patient and confirms correct insurance), insufficient DME benefits (billing team evaluates alternative payer options or patient self-pay), prior authorization required (system can trigger PA initiation automatically if configured to do so), and query errors (coordinator retries or checks the payer portal manually). Exception rates typically run 10:to:20% of total verification volume, depending on the stability of your patient population's insurance coverage.
How much does automated DME eligibility verification cost?
Pricing varies by vendor and volume tier. Clearinghouse-based eligibility checks through Waystar or Change Healthcare typically cost $0.12 to $0.45 per transaction at standard DME volumes. Agentic AI-layer solutions that add DME-specific logic, Brightree/NikoHealth write-back, and exception orchestration typically price per referral processed ($2 to $8 per referral) or as a platform subscription. At 300 referrals per month, a $4 per referral model costs $1,200 per month. Compare that against the 65:100 coordinator hours per month that the automation replaces and the denial reduction value before deciding purely on per-transaction price.
Do We Need Automated Eligibility Verification If We Already Use Brightree's Built-In Check?
Brightree's native eligibility check provides basic 270/271 connectivity that is adequate for straightforward coverage confirmation. It has limitations worth understanding: it returns basic active/inactive status rather than detailed DME benefit data; it requires coordinators to manually trigger each check rather than running automatically as part of the intake workflow; and it does not always surface HCPCS-level authorization flags or secondary insurance details. For DME operations with straightforward payer mixes and low referral volume, the native Brightree check may be sufficient. For operations processing 100 or more referrals per month, with complex Medicare Advantage or multi-payer populations, a dedicated automated verification layer with deeper benefit detail and workflow integration typically generates enough denial reduction to justify the incremental cost.
Bottom Line
Automated insurance verification is one of the most straightforward operational improvements available to DME providers because the workflow is well-defined, the transaction standards are mature, and the ROI is calculable from day one. Eligibility errors are responsible for nearly a quarter of all initial claim denials in healthcare. Most of those errors are preventable with a system that queries payers in real time, returns detailed benefit data, and writes that data directly into your order management platform without a coordinator re-entering it by hand.
The technology is not perfect. Payer coverage gaps, Medicare Advantage complexity, and coordination-of-benefits edge cases mean that human review remains necessary for a portion of every verification queue. But for DME operations processing 100 or more referrals per month, the operational case is clear: automated verification recovers staff capacity, reduces preventable denials, and confirms patient orders faster.
As DME providers continue modernizing operational workflows, many are extending eligibility automation into broader healthcare automation initiatives that include intake orchestration, payer communication, documentation workflows, and AI-assisted prior authorization management.
This shift is driving increased demand for healthtech software development services that can connect verification systems directly with platforms like Brightree, NikoHealth, and payer APIs while maintaining HIPAA compliance and operational visibility.
If you want to understand exactly where verification automation applies to your specific payer mix and workflow, the AI Readiness Audit from Clustox maps your current intake and verification workflow, identifies the highest-ROI automation opportunities, and delivers a concrete implementation plan.
Many providers evaluating verification automation are also exploring AI-driven prior authorization workflows for DME providers as part of a broader revenue cycle strategy, particularly as documentation requirements and payer complexity continue increasing across DME operations.
Ready to Eliminate Manual Eligibility Checks?
Book a consultation for an AI readiness audit. You get a full workflow map and ROI model covering eligibility verification, prior authorization, and intake automation specific to your DME operation.