For many DME providers, prior authorization creates delays long before a payer makes a decision. The real drag often starts with incomplete documentation, inconsistent payer requirements, fragmented practice management data, and repeated manual follow-up. That combination slows intake, delays delivery, and creates avoidable rework for revenue cycle teams.
Prior authorization automation is appealing because it targets those non-clinical bottlenecks. In the right setup, it can help teams organize documents, check submission readiness, track payer responses, and escalate exceptions earlier.
For many providers, the process is still heavily manual, dependent on fragmented communication, and vulnerable to staffing shortages, inconsistent payer rules, and preventable denials.
Prior authorization automation changes that equation. Instead of relying exclusively on human coordinators to manually verify eligibility, collect documentation, submit forms, and monitor payer portals, AI-driven workflows can now complete many of these steps automatically.
The result is faster turnaround times, fewer administrative bottlenecks, improved visibility, and stronger reimbursement performance.
This guide explains how prior authorization automation works in 2026, what modern DME providers should expect from automation platforms, and how operators can evaluate implementation strategies without compromising compliance, patient experience, or operational control.
Who this guide is for
This guide is written for the people who own or run prior authorization inside a US-based DME or HME provider. Specifically:
- Directors of Billing and Reimbursement who are tired of being short-staffed
- VPs of Operations who own the number on denied claims
- Owner-operators and CFOs evaluating whether AI in this category is real ROI or vendor theater
It is not written for retail-only DMEs under $5 million in revenue (the operational pain assumed in this guide does not apply at that scale), and it is not a technical reference for engineers building the agents (that is a separate piece in our DME engineering series).
This article was reviewed by Clustox Healthcare Advisory, our internal review group for DME revenue cycle and compliance content. The data points throughout this article come from primary industry sources (CAQH, CMS, AAHomecare, and HFMA), each cited inline.
Table of Contents
The state of prior authorization in DME in 2026
Prior authorization in DME is the process by which a payer reviews and approves a planned item of equipment before the provider can bill for it. In 2026, the practice is structurally broken at scale. Electronic adoption is rising but still a minority. Costs per transaction remain stubbornly high.
And the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) is forcing a multi-year transformation that providers are not, on average, ready for.
The 3 numbers frame the picture.
1. Adoption is still partial
According to the 2025 CAQH Index, electronic prior authorization adoption in medical workflows reached 40 percent in 2024, up from 31 percent in the 2023 Index. That is meaningful progress, but it also means the majority of prior authorizations in 2024 still moved through phone, fax, or portal, the three slowest modes available.
For DME specifically, electronic adoption tends to lag the broader medical average.
Two reasons: DME-specific HCPCS codes require attached clinical documentation (Letters of Medical Necessity, Certificates of Medical Necessity, prescriptions) that the X12 278 transaction has historically handled poorly, and the X12 278 attachment standard adoption sits at just 24 percent in medical workflows per the CAQH 2025 report.
2. Cost per transaction is the hidden tax
The 2024 CAQH Index put the cost of a manual prior authorization at approximately $3.41 per transaction for providers, compared to $0.05 per transaction for fully electronic submissions. That is a 98 percent unit-cost reduction, and it ignores the larger cost — the staff time consumed.
CAQH reports the time savings between manual and electronic prior auth at 14 minutes per transaction. For a DME provider processing 8,000 prior auths per year, that is roughly 1,870 staff hours, or close to one full-time coordinator’s annual capacity.
3. Turnaround drives the operational pain
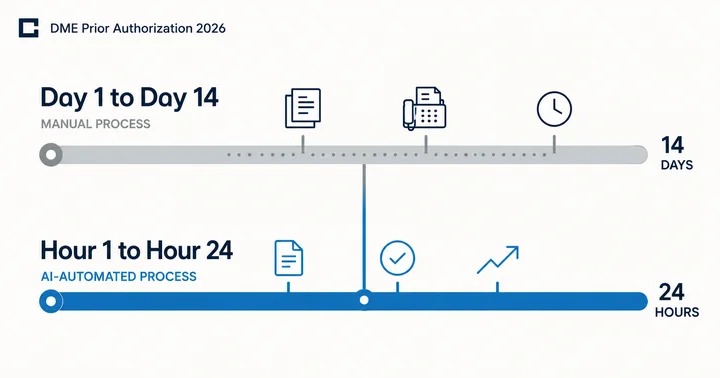
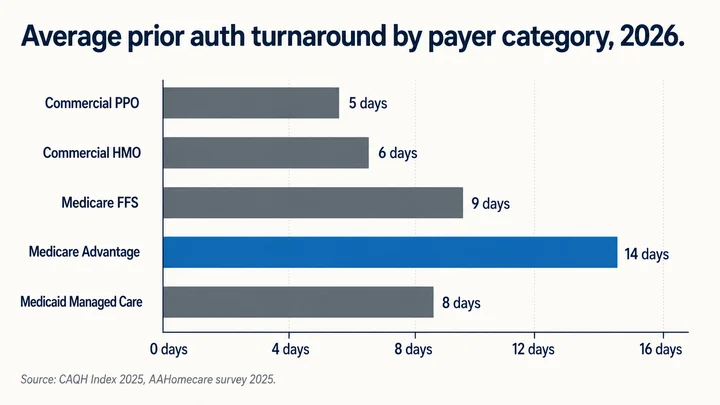
The single biggest operational pain in DME prior authorization is not cost. It is calendar time. Manual prior authorization turnaround in commercial and Medicare Advantage payers typically runs between 7 and 14 calendar days.
Medicare Advantage, in particular, is the hardest payer category, with extended review windows, complex documentation requirements, and limited transparency on submission status.
The CMS-0057-F Final Rule will compress this. Beginning January 1, 2026, impacted payers (Medicare Advantage, Medicaid managed care, CHIP, and qualified health plan issuers on the federally facilitated exchanges) must respond to standard prior authorization requests within 7 calendar days and to expedited requests within 72 hours, per CMS guidance. Full API-based compliance is required by January 1, 2027.
Why Manual Prior Authorization Breaks at Scale for DME Providers
Manual prior authorization breaks at scale because the workflow depends on too many moving parts that are hard to control manually. In DME, the problem is the combination of fragmented documentation, payer-specific rules, repeated eligibility checks, knowledge that lives in individual coordinators, and sudden volume swings. When those conditions stack up, delays and avoidable denials become part of the operating model.
Below are the five specific breakdowns that operators see most often, and the reason each one is structural rather than a staffing problem.
Documentation gathering slows the process
A DME prior authorization packet usually requires a prescription, supporting clinical notes, patient demographics, and payer-specific documentation such as an LMN or other required forms. In many organizations, those records do not live in one place. A coordinator may have to pull information from the referring physician’s EHR, the DME provider’s practice management system, faxed records, and payer portals.
That fragmentation creates a delay before the request even reaches the payer. If one required element is missing, inconsistent, unsigned, or outdated, the packet has to be corrected before submission. The result is not just slower turnaround. It is more rework, more follow-up, and more chances for the submission to fail on completeness.
Payer rules change without notice
DME providers often work across many payer types, including Medicare Advantage, Medicaid managed care, and commercial plans. Each payer may apply different documentation standards, prior authorization triggers, and submission requirements. Those rules can also change over time.
When teams manage that knowledge manually, they rely heavily on coordinator memory, local workarounds, and payer-specific habits. That works only up to a point. As payer variation increases, the risk grows that a request will be submitted with the wrong documentation set, the wrong form, or the wrong expectation of what the payer requires.
Eligibility checks expire faster than the workflow
Eligibility verification is not a one-time event. In a manual workflow, a packet may sit in queue while staff wait for corrected documentation or a response from a referring office. During that delay, the patient’s coverage or plan details may change.
That creates a common operational failure point. A packet that looked ready at intake may no longer be valid by the time it is submitted. When that happens, the denial is often tied to timing and stale information rather than to the clinical need itself.
Coordinator Turnover Reduces Workflow Consistency
Experienced coordinators often carry operational knowledge that is not fully documented, including payer preferences, escalation paths, and common documentation gaps. When those coordinators leave, that knowledge leaves with them.
New hires need time to learn payer workflows, denial patterns, and physician-office processes. During the ramp period, turnaround time and error rates usually increase unless the workflow is standardized.
Volume Spikes Overload Manual Workflows
DME order volume can rise quickly because of seasonal demand, referral growth, weather events, or payer changes. Manual teams usually cannot expand capacity at the same pace.
As the backlog grows, delays spread across intake, submission, status checks, and resubmissions. That affects both reimbursement timelines and patient service delivery.
Why These Problems Are Structural
These operational issues are not caused by one employee or one disconnected system. They come from a workflow that depends heavily on manual coordination across multiple systems, payer rules, and time-sensitive checks.
That is why many DME providers are evaluating prior authorization automation. The goal is not only to reduce manual work. It is to improve workflow consistency, reduce documentation friction, and maintain better operational control as volume grows.
What prior authorization automation actually is (and is not)
Prior authorization automation is the use of AI agent development to handle the multi-step workflow of obtaining payer approval for a DME item before delivery.
Specifically, it combines document intelligence (reading clinical notes, prescriptions, and Letters of Medical Necessity), payer-rule retrieval (looking up the specific documentation each payer requires for each HCPCS code), and structured submission (sending the package through the payer’s electronic prior auth channel or portal), with a human reviewer kept in the loop for clinical edge cases.
It is built on top of three established technical patterns: retrieval-augmented generation (RAG) for payer-rule lookup; function-calling for structured submission via the X12 278 transaction or payer APIs, and document-extraction models for reading the inbound clinical documentation. These are not experimental capabilities in 2026; they are production-grade techniques used in healthcare, financial services, and legal workflows today.
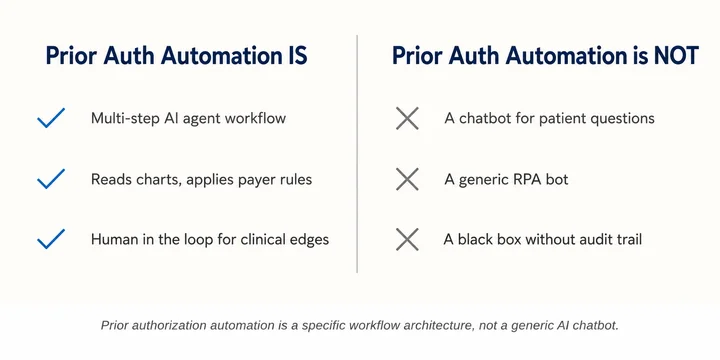
What it is
- A coordinated workflow handled by specialized AI agents, each responsible for one step of the prior auth lifecycle
- A system that reads the clinical documentation, applies payer-specific rules, and either submits the package or escalates to a human reviewer
- A compliance layer that logs every decision, preserves an audit trail, and supports HIPAA, BAA, and CMS audit defense requirements
What it is not:
- A chatbot. Prior auth automation is not a conversational interface for patients or coordinators. It is a backend workflow.
- A generic RPA bot. Robotic process automation tools that screen-scrape payer portals existed before AI agents. They are brittle, break when the portal changes, and have no comprehension of the documents they handle. AI prior authorization agents read meaning, not pixels.
- A black box. Production prior authorization automation must produce a defensible audit trail for every decision, what was read, which rule was applied, and what was submitted. This is a hard requirement, not a feature.
How It Differs From Electronic Prior Authorization (ePa)?
Electronic prior authorization, as defined by CMS and CAQH, refers to the use of standards-based transactions (the X12 278 standard and, increasingly, HL7 FHIR APIs under CMS-0057-F) to exchange prior auth requests and responses between providers and payers. ePA is the rail.
Prior authorization automation is what runs on the rail. ePA tells you how data moves between systems; automation determines what reads the data, what applies the rules, and what submits the request.
A DME can be doing electronic prior auth manually (a coordinator clicking through a payer portal) or automatically (an AI agent submitting via API). The two terms are often conflated; they should not be. We cover the distinction in more depth in our Electronic Prior Authorization for DME guide.
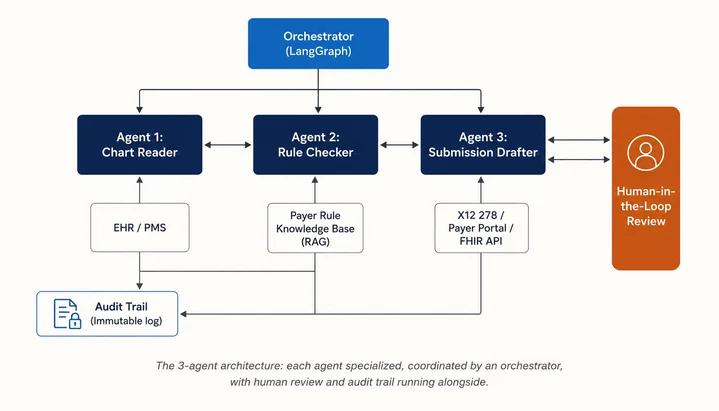
The 3-Agent Architecture: Chart Reader, Rule Checker, Submission Drafter
Most production prior authorization automation in DME is built around three coordinated agents, not a single all-purpose model. The architecture works this way because each step of the prior auth workflow has different data shapes, different failure modes, and different audit requirements.
A single agent trying to handle all three steps loses precision in each. Three agents, each specialized and coordinated by an orchestrator, keep accuracy high and the audit trail clean.
Agent 1: The Chart Reader
What it does. Reads inbound clinical documentation. Typically a Letter of Medical Necessity, Certificate of Medical Necessity, a prescription, recent clinical notes, and patient demographic information.
Extracts the structured fields needed for the prior authorization packet: diagnosis (ICD-10), HCPCS code for the requested item, clinical justification text, prescribing physician’s NPI and signature date, and patient identifiers.
The inputs it reads. Inbound documents arrive in many shapes: clean PDFs from EHR exports, scanned PDFs from physician fax machines, image-only fax pages, and, occasionally, handwritten notes. The agent uses a combination of OCR (for image-to-text), document layout analysis (to find form fields), and an LLM with a structured output schema to produce machine-readable JSON.
The outputs it produces. A structured representation of the clinical package, with a confidence score for each extracted field. Where confidence drops below a threshold (typically 92 to 95 percent on critical fields like diagnosis code and prescribing NPI), the document is flagged for human review rather than auto-progressing.
Where it struggles. Hand-written clinical notes remain the hardest input. So do legacy fax documents where the resolution is too low for reliable OCR. In those cases, the agent’s job is to flag the failure, not to guess. A confident-but-wrong extraction is worse than a flagged escalation.
Agent 2: The Rule Checker
What it does. Determines what the specific payer requires for the specific HCPCS code on the specific patient’s plan. Compares the structured package from Agent 1 against the payer’s documented prior auth rules and identifies any gaps before submission.
The inputs it reads. A vector database (the RAG layer) containing each payer’s current prior auth requirements, indexed by HCPCS code, plan type, and rule effective date. The knowledge base is updated continuously from payer policy documents, Medicare LCDs, and MAC documentation.
The outputs it produces. A go/no-go signal on whether the package is submission-ready, plus a structured list of any missing fields, supporting documentation, or signatures. The agent does not fabricate missing data; it identifies the gap and routes back to Agent 1 or to a human coordinator.
Where it struggles. Newly issued payer rules, anything in the first 30 to 60 days after publication, sometimes lag the RAG index. The mitigation is a continuously updated rules pipeline plus an override mechanism for the human reviewer to add a new rule on the fly.
Agent 3: The Submission Drafter
What it does. Packages the verified clinical content into the format the destination payer accepts and submits it through that payer’s channel. The channel might be the X12 278 transaction through a clearinghouse, the payer’s HL7 FHIR Prior Authorization API (mandatory for impacted payers by January 1, 2027 per CMS-0057-F), or, for legacy payers, a structured portal submission.
The inputs it reads. The verified package from Agents 1 and 2, plus the payer’s submission specification from a connector library.
The outputs it produces. A submitted prior auth request with a tracked submission ID, along with a status-polling subscription that monitors for the payer’s response (approval, denial, or request for more information).
Where it struggles. Payer portals that lack a stable API still require RPA-style automation, which is fragile. As CMS-0057-F drives mandatory FHIR API adoption among impacted payers, the fragility decreases. In the meantime, well-architected systems maintain a vendor-managed connector library and treat portal automation as a maintenance discipline, not a one-time integration.
The Orchestrator And The Human-In-The-Loop Layer
The three agents are coordinated by an orchestrator, in most production deployments, a framework like LangGraph or a custom state machine. The orchestrator manages state across the workflow, handles retries, and routes work between agents and humans.
The human-in-the-loop layer is not optional. For DME prior authorization specifically, 3 categories of work must always escalate to a human reviewer: clinical edge cases where the diagnosis-to-equipment fit is ambiguous; novel payer rules the system has not seen before; and any package where Agent 1’s confidence on a critical field falls below a threshold. The economics work because the human reviewer in this model handles 8 to 15 percent of volume, not 100 percent.
Every action by every agent, plus every human override, is written to an immutable audit log. The audit trail is what makes the system defensible under a CMS audit (TPE, RAC, ZPIC, or UPIC) and what allows the operator to reconstruct any decision the system made on any specific claim.
How Does it Integrate With Brightree, NikoHealth, TIMS, and Bonafide?
Prior authorization automation works alongside a DME provider’s practice management system rather than replacing it. The PMS remains the system of record for patient data, order status, eligibility, documentation, and claims activity.
For automation to work reliably, the integration has to keep data synchronized between the PMS and the prior authorization workflow. If updates are not written back correctly, teams lose visibility into submission status, attached documentation, and payer responses.
The integration approach varies across the major DME platforms.
Brightree
Brightree, owned by ResMed, is the most widely deployed DME PMS in the US market. It exposes a REST API to certified partners, supports webhook callbacks for order status changes, and has a documented integration pathway for prior auth solutions. The most common integration architecture is bidirectional: the automation reads new orders and patient context from Brightree, runs the agent workflow, and writes prior auth status, attached documentation, and approval IDs back into the Brightree order record.
The practical gotcha with Brightree integration is partner program access. The API is not a fully open developer platform; access is granted through Brightree’s partner program, which has tiered partner status and approval timelines that can extend to 90 days or longer.
NikoHealth
NikoHealth is a cloud-native DME platform that has been gaining share against Brightree, particularly among growth-stage and multi-state operators. Its API surface is more developer-friendly, with comprehensive REST endpoints and clearer documentation than Brightree’s. Integration timelines are typically shorter (4 to 8 weeks for a production-grade prior auth integration), and the platform has been deliberate about supporting modern automation vendors.
The gotcha is feature coverage. NikoHealth’s prior auth module is more recent than Brightree’s, and some legacy workflow patterns (particularly around the legacy CMN forms) require additional configuration to fully automate.
TIMS Software
TIMS is commonly used by respiratory-focused DME organizations and often supports a hybrid integration model. Many deployments combine API-based order access with file-based document exchange for clinical records and supporting documentation.
Because some TIMS environments are still deployed on-premise, infrastructure planning is usually a larger part of implementation. Integration projects may also take longer when workflows depend heavily on manual document handling.
Bonafide
Bonafide serves the mid-market DME segment with a focus on respiratory, oxygen, and complex rehab. The platform’s API is functional but less mature than NikoHealth’s, and prior auth integration generally requires direct work with Bonafide’s professional services team. The advantage for Bonafide deployments is that the customer success team is responsive and integration support is hands-on.
Operators on legacy or no PMS
A small but non-trivial share of DMEs still run on legacy on-premise systems or, in the smallest cases, on Excel and a fax machine. Prior auth automation in these environments is feasible but starts with a different question: should the operator deploy automation onto the existing rail, or use the automation deployment as the trigger to migrate to a modern PMS?
In most cases the answer is migration first, automation second. The cost of building durable integrations to a system that is itself scheduled for replacement is rarely justified.
Comparing DME Platforms for Prior Authorization Automation
This comparison highlights how the leading DME platforms differ in API access, workflow maturity, integration effort, and implementation fit for prior authorization automation.
| DME Platform | API Access | Prior Auth Module | Integration Effort | Best For |
|---|---|---|---|---|
| Brightree | Partner program REST API | Mature, widely deployed | 8-16 weeks (incl. partner approval) | Established multi-state operators |
| NikoHealth | Open REST API | Modern, configurable | 4-8 weeks | Growth-stage and cloud-native operators |
| TIMS | Hybrid API + file exchange | Functional, respiratory-strong | 8-12 weeks | Respiratory-focused mid-market |
| Bonafide | API + professional services | Functional, support-led | 6-10 weeks | Mid-market respiratory and complex rehab |
HIPAA, BAA, And Audit-Trail Requirements for AI Prior Authorization
Every component of a prior authorization automation system handles Protected Health Information (PHI). That brings the full weight of the HIPAA Security Rule, Business Associate Agreement requirements, and CMS audit defense expectations into scope.
The good news is that AI-based prior authorization automation is not especially restricted by HIPAA or by CMS; it is simply held to the same standards as any other PHI-handling system. The architecture has to be built to meet those standards from day one.
1. The HIPAA Security Rule’s Applicability
The HIPAA Security Rule’s administrative, physical, and technical safeguards apply unchanged to AI systems handling PHI.
In practice, this means:
- Encryption in transit and at rest for every data store the agents read from or write to
- Access controls including role-based access, multi-factor authentication, and audit logs of every PHI access
- Risk analysis covering the AI components, the LLM provider, the vector database, and any third-party connectors
- Incident response procedures that include AI-specific failure modes (hallucinated outputs, model drift, prompt injection)
The HHS Office for Civil Rights has not issued AI-specific HIPAA guidance separate from existing rules. The existing rules are the governing framework.
2. BAA Requirements For Every Vendor in the Chain
Every vendor that touches PHI must have a Business Associate Agreement in place with the DME provider, including the following:
- The LLM provider (OpenAI, Anthropic, AWS Bedrock, Azure OpenAI). Note that consumer-grade API access typically does not include a BAA; enterprise tiers or healthcare-specific contracts are required.
- The vector database vendor
- The cloud infrastructure provider
- Any third-party document extraction or OCR service
- The integration platform connecting to Brightree, NikoHealth, or other PMS
A common mistake during pilots is signing up for a vendor’s standard tier and then realizing on the second day of production that the standard tier does not include a BAA. The fix is expensive and slow. Audit BAA coverage before the pilot, not after.
3. Audit-trail Design
Every action taken by every agent must be logged in a way that supports reconstruction of any decision the system made. The audit log must capture, at minimum:
- The inputs the agent received (with PHI hash references rather than raw PHI in some implementations)
- The version of the model used at the time of decision
- The output the agent produced and its confidence score
- Any human-in-the-loop override and the reviewer’s identity
- The final action taken (submitted, escalated, rejected) and the timestamp
The audit trail is the defense in any CMS audit. TPE (Targeted Probe and Educate), RAC (Recovery Audit Contractor), ZPIC (Zone Program Integrity Contractor), or UPIC (Unified Program Integrity Contractor). If a claim is reviewed and the documentation chain has to be reconstructed, the audit log is what supports the case.
Where Must Humans Stay In The Loop By Policy?
Three categories of decisions should never be fully automated in DME prior authorization, regardless of how confident the AI is:
- Clinical edge cases where the diagnosis-to-equipment fit is ambiguous
- Novel payer rules the system has not previously encountered
- Final clinical content generation: the Letter of Medical Necessity content remains the prescribing physician’s responsibility, not the AI’s
This is both a compliance choice and an ethical one. The system can extract, validate, and submit. It does not author clinical justifications.
What Can You Expect From Prior Authorization Automation?
The operational impact of prior authorization automation is usually measured across three areas: turnaround time, denial prevention, and workflow scalability. Actual results depend on factors such as payer mix, documentation quality, referral intake maturity, and the structure of the provider’s existing workflow.
Turnaround Reduction
One of the most visible operational benefits of prior authorization automation is faster turnaround between order intake and payer decision.
For DME providers, turnaround time is heavily influenced by how quickly documentation moves through the workflow. Manual processes often slow down because coordinators must gather clinical notes, validate payer requirements, request corrections, and monitor status updates across multiple systems.
Automation helps reduce those delays by validating documentation earlier, identifying missing information before submission, and standardizing workflow routing. Organizations with digitized referral intake processes typically see the greatest improvement because documentation can move through the authorization workflow with fewer manual interruptions. This becomes even more effective when the authorization process is connected to strong healthcare API integration practices.
Denial Rate Impact
Documentation gaps, payer-rule mismatches, outdated eligibility information, and missing modifiers are common causes of prior authorization denials in DME workflows.
Automation helps reduce these issues through pre-submission validation and standardized rule checks. Many workflows use automation to identify missing documents, confirm required fields, and flag exceptions for human review before submission.
Headcount Impact
In most DME organizations, prior authorization automation changes how coordinators spend their time rather than eliminating the role itself.
Manual workflows often require staff to spend significant time assembling packets, checking payer requirements, following up on missing documentation, and monitoring authorization status. Automation reduces much of that repetitive coordination work and allows teams to focus more on denial management, payer communication, escalations, and complex cases that require human judgment.
Automation also helps organizations manage growth more consistently. As referral volume increases, standardized workflows reduce the operational pressure to scale entirely through additional administrative staffing. The primary operational goal is usually improved workflow stability, lower backlog risk, and better coordination across intake and authorization teams. For buyers comparing approaches, this is also a useful place to reference an AI vendor evaluation checklist.
What are the CMS rules and Medicare-specific considerations?
The CMS rule set governing prior authorization in DME has changed materially in the past 24 months, and the next 24 will change it further. Operators evaluating prior auth automation need to understand both the current rules and the trajectory.
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F)
Issued by CMS in January 2024, CMS-0057-F requires impacted payers, Medicare Advantage organizations, state Medicaid and CHIP agencies, Medicaid and CHIP managed care plans, and Qualified Health Plan issuers on the federally facilitated exchanges to implement specific prior authorization improvements on a phased timeline.
- By January 1, 2026: Impacted payers must process standard prior authorization decisions within 7 calendar days (down from 14 days previously for many plans) and expedited decisions within 72 hours. Public reporting of prior auth metrics begins.
- By January 1, 2027: Impacted payers must implement a Prior Authorization API based on HL7 FHIR standards, plus a Patient Access API, Provider Access API, and Payer-to-Payer API.
The rule does not directly regulate providers, but the practical impact on DMEs is significant. The compressed payer response timeline means slow internal workflows that previously had cover are now exposed. A DME that takes 5 days to assemble and submit a packet, then waits 14 days for a response, used to look like the payer was the bottleneck. After January 2026, when the payer must respond in 7 days, the DME’s internal 5-day delay is half of the total turnaround.
Medicare Fee-for-Service and the DME MAC prior authorization requirements
For Medicare Fee-for-Service, prior authorization for DME has been required since 2017 for a defined list of HCPCS codes, expanded several times since.
The current required list is maintained by CMS and the four DME MACs (CGS, Noridian, Palmetto, and CGS Administrators). The required list includes most power mobility devices, lower-limb prosthetics, certain pressure-reducing support surfaces, and selected respiratory items.
The MAC-specific Local Coverage Determinations vary in their documentation requirements. A power wheelchair prior auth in the CGS jurisdiction is not identical to the same item in Noridian jurisdiction. Prior auth automation systems must maintain MAC-specific rule sets, not just a single Medicare rule set.
Medicare Advantage prior auth specifics
Medicare Advantage is the hardest payer category for DME prior auth. Plans set their own prior auth requirements within the bounds of CMS rules, and the requirements vary widely across the major MA carriers. The CMS-0057-F rule changes the response timeline for MA plans starting January 2026, but does not standardize their documentation requirements.
Practically, this means that any AI prior auth system worth deploying must have first-class support for MA payer rules, including ongoing updates as plans modify their requirements.
What Are The Common Implementation Mistakes (And How To Avoid Them)
Operators evaluating prior auth automation in 2026 are doing so at the end of a hype cycle. There are vendor pitches in this market that are excellent and vendor pitches that are theater. The seven mistakes below are the failure modes we see most often.
1. Starting Without A Clean PMS Data Layer
Prior auth automation reads from and writes to the PMS. If the PMS data is incomplete, miscoded, or fragmented across systems that do not talk to each other, the automation cannot succeed on top of it. The first 30 days of any serious engagement should include a PMS data audit. Operators who skip this step typically discovers the problem at week 8, when the integration looks complete but the automation is producing 40 percent failure rates because the patient records it is reading are unreliable.
2. Choosing The Wrong First Payer To Pilot On
The instinct is to pilot on the hardest layer, because that is where the pain is greatest. The better choice is to pilot on a payer with a reasonable rule set, a stable submission channel, and adequate volume. A pilot on a fringe Medicaid managed care plan with 200 monthly transactions and inconsistent rules will not produce useful signal. A pilot on a commercial PPO or a single MAC region typically does.
3. Underestimating Change Management For Billing Staff
The team that has been doing prior auth manually for years has developed institutional knowledge that the automation will need to absorb, and they need to be brought into the deployment as collaborators, not as the audience for a fait accompli. The operators who succeed typically involve their senior coordinator in the design of the human-in-the-loop escalation rules. The operators who struggle typically announce the deployment without that involvement and then face quiet resistance for months.
4. Skipping The Human-In-The-Loop Design
A vendor that pitches “fully autonomous prior auth” in DME is selling either a fiction or a compliance risk. The architecture has to assume human escalation as a first-class capability, not as a fallback. The escalation rules, what triggers a human review, how routing works, what the reviewer sees — should be designed in week one, not added in month six.
5. Choosing A Vendor That Uses One General-Purpose LLM For Everything
A single general-purpose model handling document extraction, rule lookup, and submission drafting is architecturally simpler but operationally weaker. Each step has different precision requirements, different latency budgets, and different failure modes. Vendors that have invested in the three-agent (or multi-agent) architecture typically produce more consistent results and have cleaner audit trails.
6. Not Building The Audit Trail From Day One
Audit trails added retroactively are always incomplete. CMS audit defense, internal compliance review, and any regulatory inquiry depend on a complete, immutable record of what the system did and why. Build the audit log into the first deployed component; do not treat it as a phase-two feature.
7. Treating It As A Tool Purchase Rather Than A Workflow Program
Prior auth automation is not a SaaS license you turn on. It is a workflow transformation that touches intake, documentation, billing, denial management, and clinical operations.
The engagements that succeed are structured as programs with a 90-day discovery and pilot phase, a 90-day production rollout, and a continuous operations phase. The engagements that fail are structured as one-time integrations with a defined end date.
Frequently Asked Questions
How Long Does Prior Authorization Take With AI vs. Manual Processing?
Manual prior authorization typically takes 7–14 days. AI-assisted workflows can reduce turnaround times to 1–3 days, with some expedited requests resolved the same day. Results depend on payer responsiveness and documentation quality.
Is AI-Submitted Prior Authorization HIPAA-Compliant?
Yes, provided the system includes HIPAA safeguards such as Business Associate Agreements (BAAs), role-based access controls, audit logging, encryption, and secure infrastructure. AI systems are subject to the same HIPAA requirements as any other PHI-handling platform.
Does Medicare Allow AI-Submitted Prior Authorizations?
Yes. CMS does not prohibit AI-assisted prior authorization submissions. The submission must still meet existing documentation and transaction standards, while the prescribing physician remains responsible for the clinical content.
How Does AI Handle Letters of Medical Necessity (LMNs)?
AI systems can validate LMNs by checking for required elements such as physician signatures, diagnosis codes, NPIs, and clinical justification. If information is missing or inconsistent, the case is escalated for human review rather than auto-submitted.
What HCPCS Codes Require Prior Authorization in 2026?
Medicare requires prior authorization for selected HCPCS codes, including many power mobility devices, prosthetics, support surfaces, and respiratory products. Commercial and Medicare Advantage plans often maintain broader authorization requirements that vary by payer.
How Much Does Prior Authorization Automation Cost?
Costs vary by vendor and deployment scope. Most projects include:
- Discovery and audit phase
- Pilot implementation
- Full production rollout
- Ongoing support or per-transaction pricing
Pricing can range from small pilot engagements to enterprise-scale operational deployments.
What Is the Typical ROI of AI Prior Authorization for DME?
ROI is usually driven by:
- Faster reimbursement cycles
- Lower denial rates
- Reduced administrative overhead
- Improved staff productivity
Many DME providers report ROI payback periods between 6–14 months, depending on workflow volume and operational maturity.
Does AI Replace Billing Staff or Augment Them?
Most DME providers use AI to augment staff, not replace them. Automation handles repetitive administrative tasks so coordinators can focus on escalations, appeals, complex cases, and payer management.
What Happens When AI Is Uncertain About a Submission?
The workflow escalates the case to a human reviewer. Modern systems use confidence thresholds and route incomplete or low-confidence submissions for manual verification before anything is sent to the payer.
How Accurate Is AI at Reading Clinical Documentation?
Accuracy depends on document quality. Structured fields from clean EHR-generated PDFs are often extracted with very high accuracy, while scanned faxes or handwritten notes require more human oversight. Critical clinical decisions should always include human review.
Conclusion
Prior authorization remains one of the largest operational pressure points in the DME industry. As payer requirements become more complex and staffing challenges continue across healthcare operations, manual workflows are becoming increasingly difficult to sustain at scale.
Automation does not replace operational expertise. Instead, it enables experienced teams to spend less time on repetitive administrative coordination and more time on higher-value work such as exception handling, denial prevention, payer escalation, and patient service.
For DME providers evaluating AI-driven workflows in 2026, the question is no longer whether prior authorization automation will become standard. The real question is how quickly organizations can adopt the right operational model without compromising compliance, reimbursement performance, or workflow visibility.
At Clustox, we are seeing growing demand from DME operators for practical AI implementations that integrate with existing workflows rather than disrupt them. The most successful deployments are not built around replacing teams but around creating more scalable, audit-ready, and operationally resilient authorization processes that support long-term growth.
As CMS timelines tighten and payer interoperability requirements continue evolving, providers that modernize their prior authorization workflows early will be better positioned to reduce delays, improve operational consistency, and protect revenue performance in the years ahead.
This article is for DME providers, operations leaders, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, accreditation standards) are accurate as of the review date; regulations change frequently and providers should consult primary sources or qualified counsel for current requirements.