
Autonomous healthcare AI uses software agents to complete operational work, such as eligibility checks, prior authorization, and re-supply outreach, with limited human oversight instead of full manual effort. An AI-first operation designs these workflows around agents from the start. You keep people on judgment, exceptions, and care-adjacent decisions.
You have heard the phrase “AI-first” in every vendor deck this year. Most of the time it means a chatbot bolted onto an old workflow. That is not what this article is about.
This guide is for the people who own the operational result. If you are a COO watching headcount grow faster than revenue, a CTO who needs a build that survives production, or an owner tired of hiring people to do work software should handle, this is written for you.
You will get a working definition of autonomous healthcare AI, a clear picture of what AI-first operations look like inside a real back office, the architecture behind agentic AI operations, the numbers that actually move, and an honest account of the limits.
What this article covers
- A plain definition of autonomous healthcare AI and AI-first operations.
- Which workflows go autonomous first, and which stay human.
- The agentic architecture and the human-in-the-loop checkpoints.
- The operational numbers, with sourced statistics.
- A phased rollout plan, the real risks, and a build-versus-buy-versus-partner view.
What Is Autonomous Healthcare AI?
Autonomous healthcare AI is a system of software agents that plan and complete operational tasks end to end, with humans setting the rules and reviewing exceptions. It does not mean a workflow with no people. It means the routine path runs without a person clicking through every step, while staff handle judgment calls, edge cases, and anything that touches clinical or financial risk.
The word “autonomous” does real work here, so define the boundary. Autonomy is scoped. An agent gets a goal, a set of tools, a set of guardrails, and a point where it must stop and ask. A good system is measured by how often it finishes the routine work correctly, not by how often it acts without a human.
Table of Contents
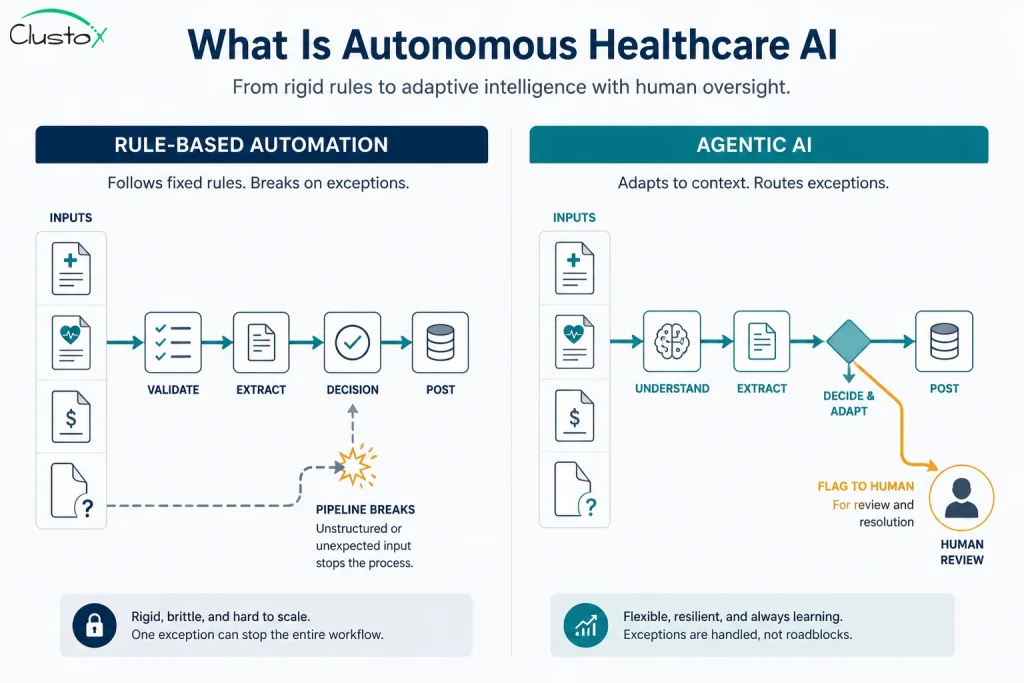
There is a useful contrast with the automation you already run. Traditional automation follows fixed rules and breaks the moment reality changes. Agentic AI operations read context, make a decision, use a tool, check the result, and adjust.
That difference is the whole story, so it deserves a table.
| Dimension | Traditional automation (RPA, macros) | Autonomous healthcare AI (agents) |
|---|---|---|
| Decision logic | Fixed if-then rules | Reads context, reasons, then acts |
| Handling variation | Breaks on any layout or rule change | Adapts to new inputs within guardrails |
| Unstructured data | Cannot read charts, faxes, or notes well | Reads notes, faxes, and documents |
| When it gets stuck | Fails silently or stops | Flags an exception for a human |
| Maintenance | Constant rule rewrites | Updates to prompts, tools, and policy |
Keep one thing in mind as you read on. Autonomy is a spectrum, not a switch. Most healthcare operations land in the middle, where agents do the heavy lifting and people own the calls that matter.
Why ‘AI-First Operations’ Is Different From Adding A Chatbot
AI-first is an operating posture, not a feature. The distinction decides whether you get a pilot that dies or a system that runs your Monday morning.
When you add a chatbot, you keep the old process and put a thin layer on top. The work still flows the way it did in 2018. When you go AI-first, you redesign the workflow so an agent owns the default path and a person owns the exception. The org chart, the metrics, and the software all assume agents do the routine volume.
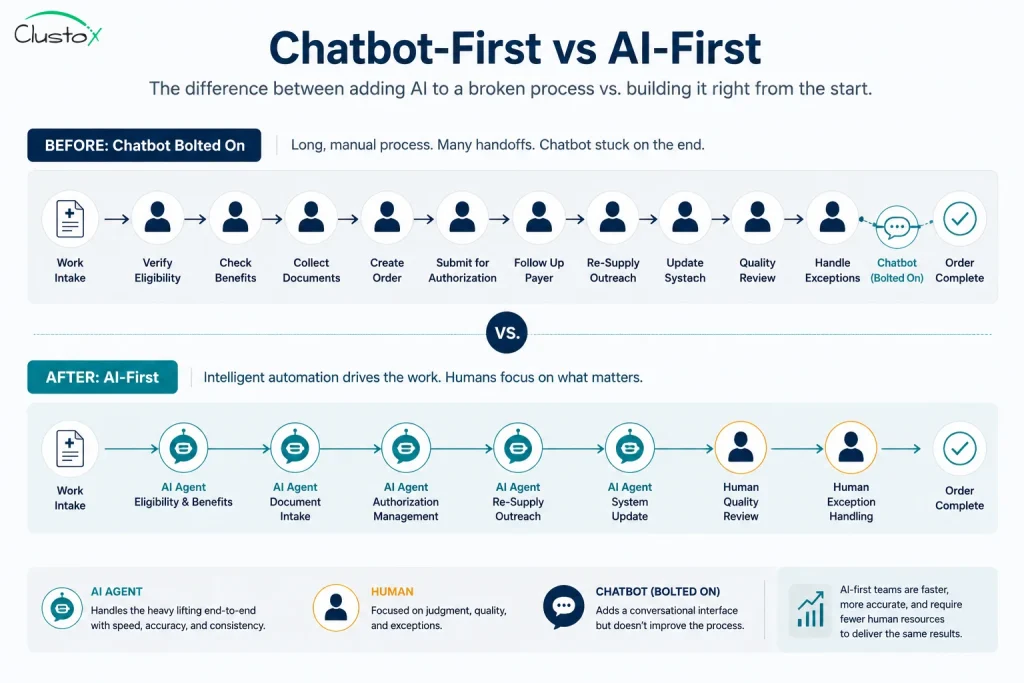
Here is the practical test. In a chatbot-first shop, removing the AI changes very little, because it was decoration. In an AI-first shop, removing the agents would force you to rehire a team because the agents carry real load. That is the line you are trying to cross.
Three shifts separate the two postures, and each one shows up in how you staff and measure the work.
- Default path flips. The agent runs the task first. The human reviews flagged items, not every item.
- Metrics change. You stop measuring tickets closed per person and start measuring exception rate, accuracy, and cost per completed transaction.
- Roles change. Your best operators move from data entry to building rules, reviewing edge cases, and improving the agents.
This is also where the scale of the opportunity becomes clear. U.S. national health spending reached $5.3 trillion in 2024, about 18% of the economy, and a large share of that is administrative work that never touches a patient.
What AI-First Actually Looks Like Inside A Healthcare Operation
Theory is easy. The useful question is what changes on the floor. This section walks through the workflows that go first and a realistic day in an AI-first back office.
Not every workflow is a candidate, so start with the ones that have high volume, clear rules, and a measurable result.
The list below reflects where durable medical equipment (DME) and similar healthcare operations get the fastest return.
The Workflows That Go First
Before selecting automation candidates, many providers use a DME Workflow Automation Checklist to identify repetitive, high-volume tasks that are suitable for AI-driven workflows.
These workflows share a pattern. They are repetitive, they sit on structured or semi-structured data, and a wrong answer is recoverable through human review.
- Eligibility and benefits verification. Agents check coverage against the payer, read the response, and post the result, then flag mismatches.
- Prior authorization. Agents read the chart, check the payer rule, assemble the documentation, and draft the submission for a human to approve.
- Documentation compliance. Agents confirm that a Letter of Medical Necessity and required fields are present before a claim moves. This is where CMN Automation helps reduce manual document reviews and ensures supporting documentation is complete before submission.
- Denial management. Agents triage denials, group them by root cause, and draft appeals for soft denials. Modern Denial Management Software helps teams automate this process, prioritize high-value claims, and accelerate appeal workflows.
- Patient intake and re-supply outreach. Agents handle CPAP re-supply contact, capture responses, and update the system of record.
Prior authorization deserves a flag because it is both the biggest pain and a regulated workflow. Manual prior authorization is slow, and adoption of fully electronic submission is still low across the industry.
To see how this lands day to day, picture the back office of a multi-state DME provider running a system of record like Brightree or NikoHealth. The next section describes a normal Tuesday.
A Day In An AI-First DME Back Office
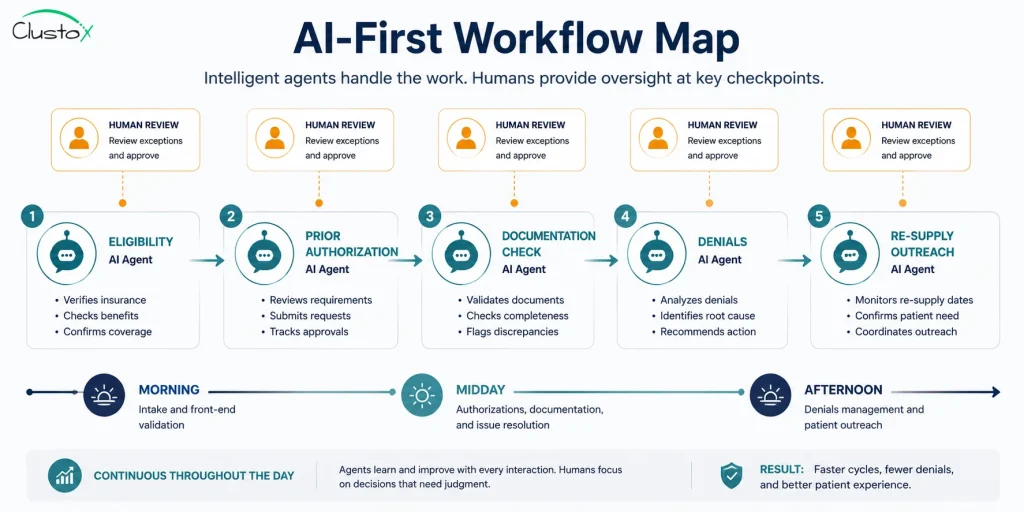
The shift starts, and the queue is already moving. Overnight, agents verified eligibility on the new orders and posted clean results. Your specialist opens a dashboard, not an empty inbox.
By mid-morning, the prior authorization agent has drafted submissions for the day’s new equipment orders. It read each chart, matched the payer policy, and attached the documentation. Your specialist reviews the flagged drafts, approves most, and corrects two where the clinical notes were thin. She spends her time on the two, not the fifty.
In the afternoon, the denial agent has sorted the day’s denials by reason. Soft denials already have draft appeals waiting. The re-supply agent has reached 300 CPAP patients by text, logged the responses, and queued the ones who need a callback. None of this required a person to start it.
The point is not that people disappear. The point is that people now do the work that needs a brain, and the volume work runs itself within the guardrails you set.
The Architecture Behind Agentic AI Operations
If you own the build, you need to know what sits under the hood. This section is for the CTO and the technical evaluator, though the structure is simple enough for any operator to follow.
Agentic AI operations are not one giant model doing everything. They are a set of focused agents, each with a narrow job, coordinated by an orchestration layer. That design keeps each step testable and keeps failures contained.
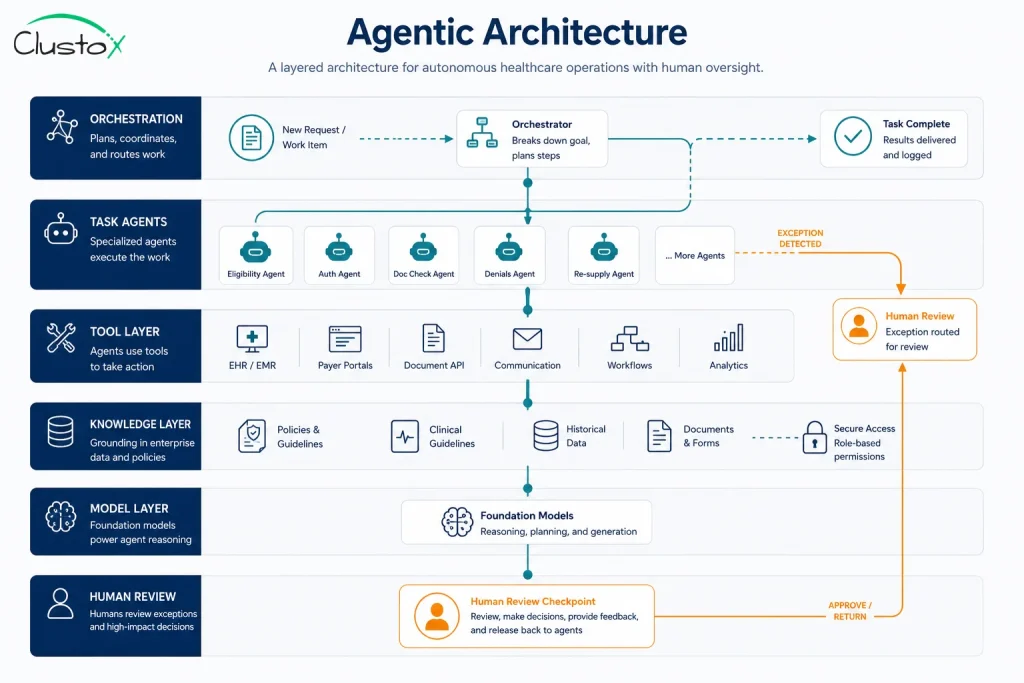
Before the components, the principle. Each agent should do one thing, use defined tools, and hand off cleanly. The orchestration layer routes work, enforces policy, and decides when to call a human. The table below shows the core pieces.
How The Agents Are Structured
Think of it as a small team with a manager. The manager assigns work, the specialists execute, and a reviewer checks the output before it leaves the building.
| Component | Job | Example in healthcare ops |
|---|---|---|
| Orchestrator | Routes tasks, enforces guardrails, manages handoffs | Frameworks such as LangGraph coordinating multi-step work |
| Task agents | Execute one workflow each | Eligibility agent, prior auth agent, denial agent |
| Tool layer | Connects agents to systems | APIs into Brightree, NikoHealth, payer portals, X12 278 |
| Knowledge layer | Supplies context and policy | Retrieval (RAG) over payer rules and HCPCS references |
| Model layer | Reasoning and language | Large language models hosted on AWS Bedrock or similar |
| Review layer | Human checkpoints and audit log | Exception queue, approval steps, full trace of actions |
The model is only one layer, and that surprises people. Most of the engineering effort goes into the tool layer, the policy guardrails, and the evaluation harness, because that is what makes the system reliable in production.
Reliability also depends on knowing where a person must stay involved. That boundary is a design decision, not an afterthought, so it gets its own section.
Where Humans Stay In The Loop
You decide the checkpoints up front. A clean rule is to keep a human on anything that creates clinical, legal, or financial risk and to let agents run the rest under audit.
- Approval gates. An agent drafts a prior authorization or appeal, which a person approves before submission.
- Confidence thresholds. When the agent is unsure, it routes to a human rather than guessing.
- Exception queues. Anything outside the rules lands in a queue a person owns.
- Audit trails. Every agent action is logged, so you can trace and explain any decision.
On data protection, treat this as non-negotiable. Any system touching protected health information must run on a HIPAA-compliant architecture, with access controls, encryption, and a Business Associate Agreement in place. Confirm the specific controls with your security and compliance reviewers before launch.
The Numbers: What Autonomous Healthcare AI Changes
Outcomes decide budgets, so this section is about what moves. The figures here come from industry benchmarks and the directional ranges teams report when they automate these workflows.
Start with the macro signal. Automation already saves the system real money, which tells you the direction of travel is set.
Automation and electronic data exchange helped U.S. healthcare avoid an estimated $258 billion in administrative costs in 2024, according to the 2025 CAQH Index.
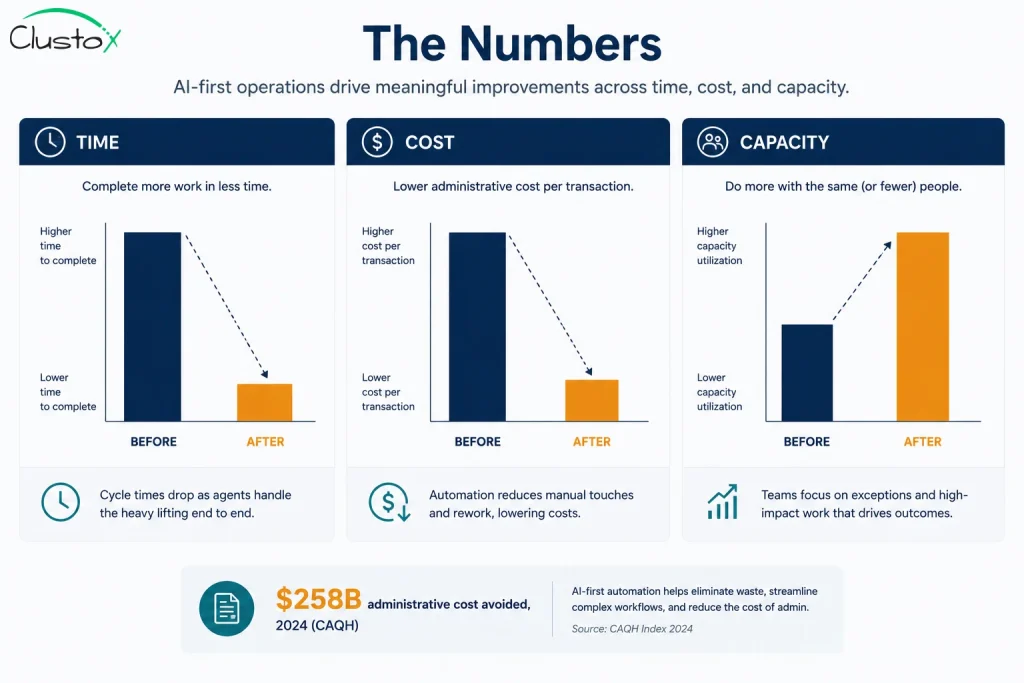
At the operation level, the gains show up in three places: time, cost, and capacity. These improvements directly impact overall DME Revenue Cycle Management, helping providers reduce administrative overhead while improving reimbursement performance. The table below frames the kind of before-and-after picture teams aim for. Treat these as illustrative targets to validate against your own baseline, not guarantees.
| Operational metric | Manual baseline (typical) | AI-first target (directional) |
|---|---|---|
| Prior auth turnaround | Several days, manual touch on each | Same or next day on routine cases |
| Staff time per transaction | High, every item handled by a person | Low, people handle flagged exceptions |
| Throughput per FTE | Capped by headcount | Scales with volume, not headcount |
| Soft denial recovery | Inconsistent, often abandoned | Systematic, drafted appeals queued |
| After-hours coverage | None or expensive | Agents run intake and outreach overnight |
A word of caution on numbers. Be skeptical of any vendor that quotes a precise percentage for your business before they have seen your data. The honest move is to measure your current baseline, run a scoped pilot, and compare. The ranges only mean something against your own starting point.
The headcount math is the part owners care about most. AI-first does not usually cut your team on day one. It lets you take on more volume without adding people, and it moves your existing staff to higher-value work. That is how the headcount-to-revenue ratio improves.
How To Move Toward AI-First Operations Without Breaking Things
Ambition fails when it skips sequencing. You move toward AI-first one workflow at a time, with a baseline, a guardrail, and a measure for each step.
The single biggest mistake is trying to automate everything at once. Pick one high-volume workflow, prove it in production, then expand. A scoped start also gives you a real number to show the board.
Here is a sequence that works in practice. It assumes you already have a system of record with API access and data that is not trapped in PDFs or one person’s head.
A Phased Rollout
Each phase ends with a decision: keep going, adjust, or stop. That structure keeps the risk small and the learning fast.
- Audit and baseline. Map one workflow end to end, measuring current time, cost, and error rate. This is your before number.
- Pilot one workflow. Build an agent for the single workflow, keep a human on every output, and run it on real volume.
- Tune the guardrails. Adjust confidence thresholds and exception rules until the flagged rate is sensible and accuracy holds.
- Expand the autonomy. Let the agent auto-complete the clear cases, keep humans on the flagged ones, and watch the metrics.
- Add the next workflow. Repeat with the next-highest-volume process, reusing the orchestration and review layers.

Phasing only works if you watch the right signals. The next section lists the metrics that tell you the system is healthy or drifting.
What To Measure
Vanity metrics will lie to you. Track the numbers that connect to cost, quality, and trust.
- Exception rate. What share of items does the agent flag for a human? Too high means the agent is weak. “Too low” can mean it is overconfident.
- Accuracy on a reviewed sample. Audit a regular sample of completed work to confirm quality holds as volume grows.
- Cost per completed transaction. The number that proves the business case against your manual baseline.
- Turnaround time. How fast the routine path now completes, end to end.
- Time to resolve exceptions. How quickly your team clears the flagged queue, which protects service levels.
The Limits And Risks You Should Plan For
Anyone who tells you this is risk-free is selling. The systems are strong on volume work and weak in predictable places, and naming those places up front is how you stay out of trouble.

The risks are manageable, but only if you design for them. The table below pairs the common failure modes with the control that contains each one.
| Risk | What it looks like | How you contain it |
|---|---|---|
| Wrong answers (hallucination) | Agent drafts an incorrect submission | Human approval gates, confidence thresholds, sample audits |
| Data privacy exposure | PHI handled outside compliant boundaries | HIPAA-compliant architecture, encryption, access controls, BAAs |
| Regulatory change | A payer or CMS rule shifts | Policy in the knowledge layer, fast update path, SME review |
| Pilot that never ships | A demo that never reaches production | Scope to one workflow, set a go-live date, measure in production |
| Staff resistance | Team distrusts or bypasses the agents | Involve operators early, keep them on judgment work, show the wins |
| Over-automation | Removing humans from calls that need them | Keep clinical, legal, and financial decisions with people |
Two limits are worth stating plainly. First, autonomous healthcare AI reduces manual effort and error rates, it does not erase errors, so the review layer is permanent. Second, an agent should never make a clinical judgment. It supports the operations around care decisions, and the decision stays with qualified people.
Honesty about the hard parts is not a weakness in the pitch. It is the reason the system earns trust on the floor and survives its first bad week.
Build vs. Buy vs. Partner For Autonomous Healthcare AI
Once the case is clear, the next decision is how to get there. There are three paths, and the right one depends on your engineering depth, your timeline, and how specific your workflows are.
None of these is universally correct. The table lays out the honest trade-offs so you can match the path to your situation.
| Path | Best when | Trade-off to watch |
|---|---|---|
| Build in-house | You have senior AI engineers and time | Hiring and time-to-production risk; ongoing maintenance |
| Buy a product | Your workflow is standard and the tool fits | Generic fit, limited control, integration gaps with your stack |
| Partner to engineer | Workflows are specific and you want production fast | You must pick a partner who ships, not one who slides |
A practical filter helps here. If your workflows are highly specific to your payers, your software, and your patient mix, an off-the-shelf product rarely fits cleanly, and building from scratch is slow unless you already have the team. That is the gap a focused engineering partner closes.
Whatever path you choose, insist on production, not slides. Ask to see architecture, evaluation methods, and a working result on real volume. A pilot that never reaches production is the most expensive outcome of all.
Frequently Asked Questions (FAQs)
Is autonomous healthcare AI HIPAA compliant?
It can be, and it must be, if it touches protected health information. Compliance comes from the architecture, not the model alone. You need encryption, access controls, audit logging, and a Business Associate Agreement with any vendor in the data path. Confirm the specific controls with your security and compliance reviewers before launch.
Which healthcare operations should you automate first?
Start with high-volume, rule-heavy workflows where a wrong answer is recoverable through review. Eligibility verification, prior authorization, documentation checks, denial management, and re-supply outreach are common first picks. Pick one, prove it in production, then expand. A scoped start gives you a real number before you commit further.
Does AI-first operations mean replacing your staff?
Usually not on day one. AI-first lets you take on more volume without adding headcount, and it moves your existing team from data entry to judgment and exception work. The goal is a better headcount-to-revenue ratio, not an empty office. Your best operators become the people who improve and oversee the agents.
How long does it take to move to AI-first operations?
A single scoped workflow can reach production in weeks, not years, when your data and integrations are ready. The full shift across multiple workflows is a phased program measured in months. The timeline depends on data quality, system access, and how many workflows you take on. Sequencing one at a time keeps the risk small.
How do you measure ROI on agentic AI operations?
Measure cost per completed transaction against your manual baseline, then track throughput per person, turnaround time, and exception rate. Audit a sample of completed work to confirm accuracy holds as volume grows. The clearest proof is handling more volume without adding people. Always compare against a baseline you measured before the pilot.
Conclusion: Where AI-First Operations Actually Starts
Autonomous healthcare AI is not a chatbot and not a science project. It is a system of focused agents that run your routine operational volume, with your people on judgment, exceptions, and anything that touches care or money. AI-first is the posture where agents own the default path and humans own the calls that matter.
The takeaways are simple. Define autonomy as scoped, not human-free. Start with one high-volume workflow, measure a real baseline, and expand from proof. Build the human-in-the-loop checkpoints and the HIPAA-compliant architecture from the start. Be honest about the limits, because that is what makes the system trustworthy in production.
The cost of waiting is quiet but real. Every month on manual workflows is another month of headcount growing faster than revenue and capacity capped by hiring. The operators moving now are not chasing a trend. They are taking the administrative load off their teams and putting it on software that runs overnight.
You do not have to commit to a year-long program to find out if this fits. You start with one workflow and one honest measurement.
Ready to see what AI-first looks like for your operation?
Book a fixed-price AI Readiness Audit. We map one high-volume workflow end to end, identify where agents fit, and hand you a baseline and a plan you can act on. No slides, a working assessment.