Healthcare prior authorization is the approval a health plan requires before it will pay for a treatment, medication, or piece of equipment. For years that approval could take up to 14 days. New federal rules and automation are now pushing the process toward faster decisions and, in some cases, toward near real-time approvals.
If you run a provider organization or oversee its operations, this matters to you in three ways at once. It shapes how long patients wait. It decides how many staff hours you spend chasing paperwork. It affects how fast you get paid.
The pressure is building from two directions at the same time. Patients and physicians have pushed hard for reform, and federal regulators have answered with firm deadlines. Meanwhile, the technology to automate the slow parts of the process has finally caught up. The result is a rare moment when policy and capability point the same way.
This guide is written for that moment. It walks through the full picture, from how the process works today to where it is heading, and it stays focused on what you can do about it. Read it as a working reference, not a think piece. Every section is built to help you make a decision or take a step.
What This Guide Covers
Here is the ground this guide covers, in order.
- How healthcare prior authorization works and why it causes delays.
- The real operational and financial cost of those delays.
- What the CMS-0057-F rule changes are and by when.
- How manual, electronic, and AI-assisted workflows compare.
- How AI moves the process toward real-time approvals and where humans stay in control.
- A practical roadmap to prepare your own workflow.
- The common mistakes to avoid along the way.
What Is Healthcare Prior Authorization, and Why Does It Slow Care Down?
Prior authorization sits between a clinical decision and the care a patient receives. Your provider recommends something, and the payer reviews it before agreeing to pay. The intent is cost control. The side effect is delay.
The process touches almost every part of healthcare operations. It applies to imaging, specialty drugs, elective procedures, and durable medical equipment. When it works, it is invisible. When it stalls, patients wait and staff chase records.
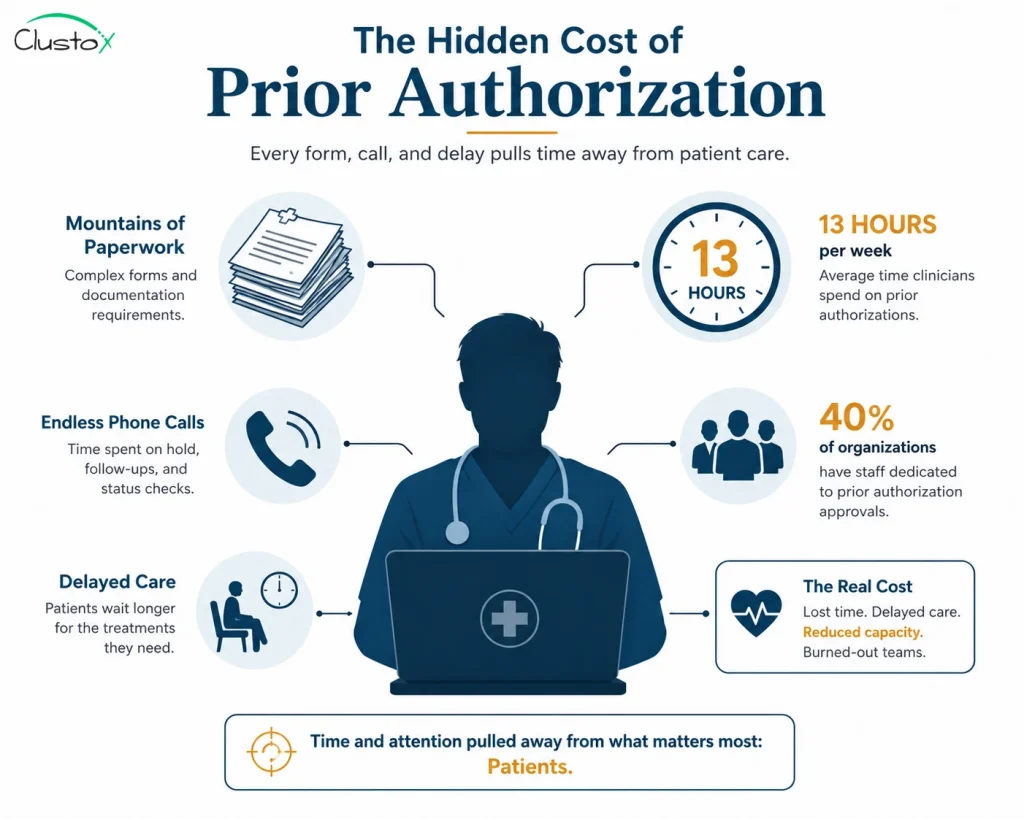
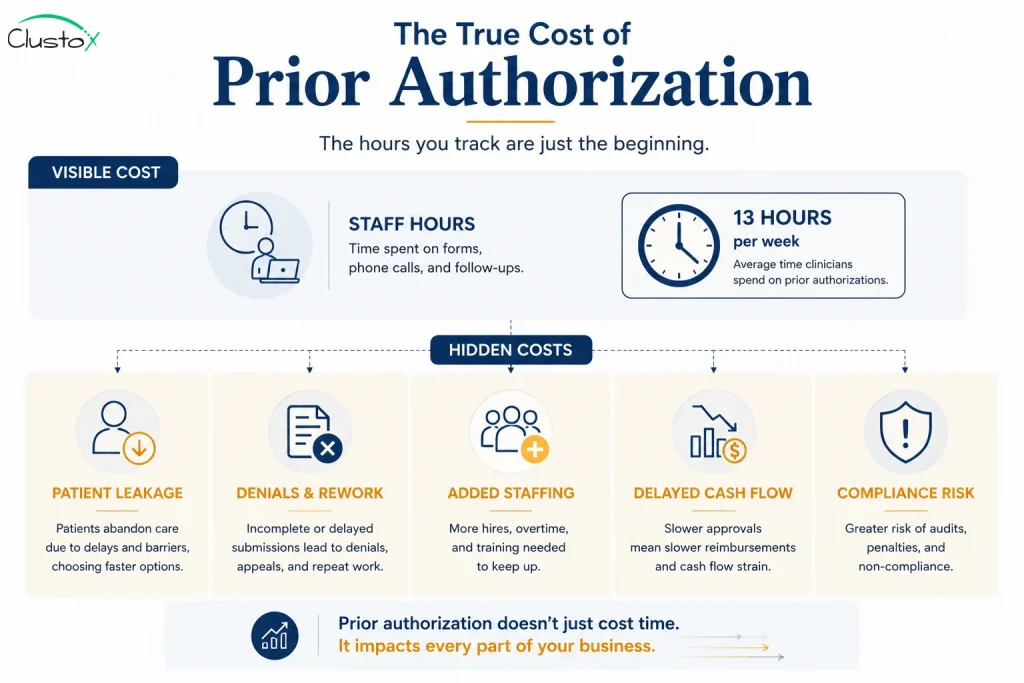
The administrative load is heavy. Physicians and their staff spend an average of 13 hours each week on prior authorization, according to the 2025 AMA Prior Authorization Physician Survey (AMA, 2026). That is more than a full day of work, every week, on approvals alone.
Table of Contents
The cost is not measured only in hours. It also shows up in patient outcomes and staff morale.
How Prior Authorization Delays Affect Patients and Providers
Delays carry real consequences. Patients postpone treatment, abandon prescriptions, or end up in the emergency room when a condition worsens. For providers, the workload pulls trained staff away from care and into data entry and follow-up calls.
The staffing burden is large enough that 40% of physicians now employ staff who work exclusively on prior authorization, per the AMA (2026). For a growing practice, that is headcount added to manage a process, not to serve more patients.
The True Cost of Prior Authorization Delays
The hours spent on approvals are only the visible cost. The deeper cost shows up in revenue, retention, and reputation. For an operations leader, prior authorization is a financial control point, not just an administrative chore.
Every stalled request ripples outward. A patient who waits too long may walk away, and that lost case takes its revenue with it. An incomplete submission gets denied, then reworked, which doubles the labor on a single request. As volume grows, the only way to keep pace manually is to keep hiring, so your cost base rises in step with your caseload.
Cash flow feels it too. You cannot bill for a service until it is authorized and delivered, so a slow authorization is a slow payment.
The table below shows where the cost tends to hide.
| Cost Area | How Prior Authorization Delays Drive It |
|---|---|
| Patient leakage | Patients abandon treatment or go elsewhere when approvals stall. |
| Denials and rework | Incomplete submissions get denied, then reworked and resubmitted. |
| Staffing | Volume growth forces you to add coordinators just to keep pace. |
| Cash flow | You cannot bill until the service is authorized and delivered. |
| Compliance risk | Manual tracking makes the new reporting and timeline rules harder to meet. |
It is worth being fair to the payers here. Not every denial is wrong. Many requests truly do arrive missing a document or a code, and a denial is the predictable result. That is exactly the kind of problem automation is good at preventing, because it catches the gap before the request ever goes out.
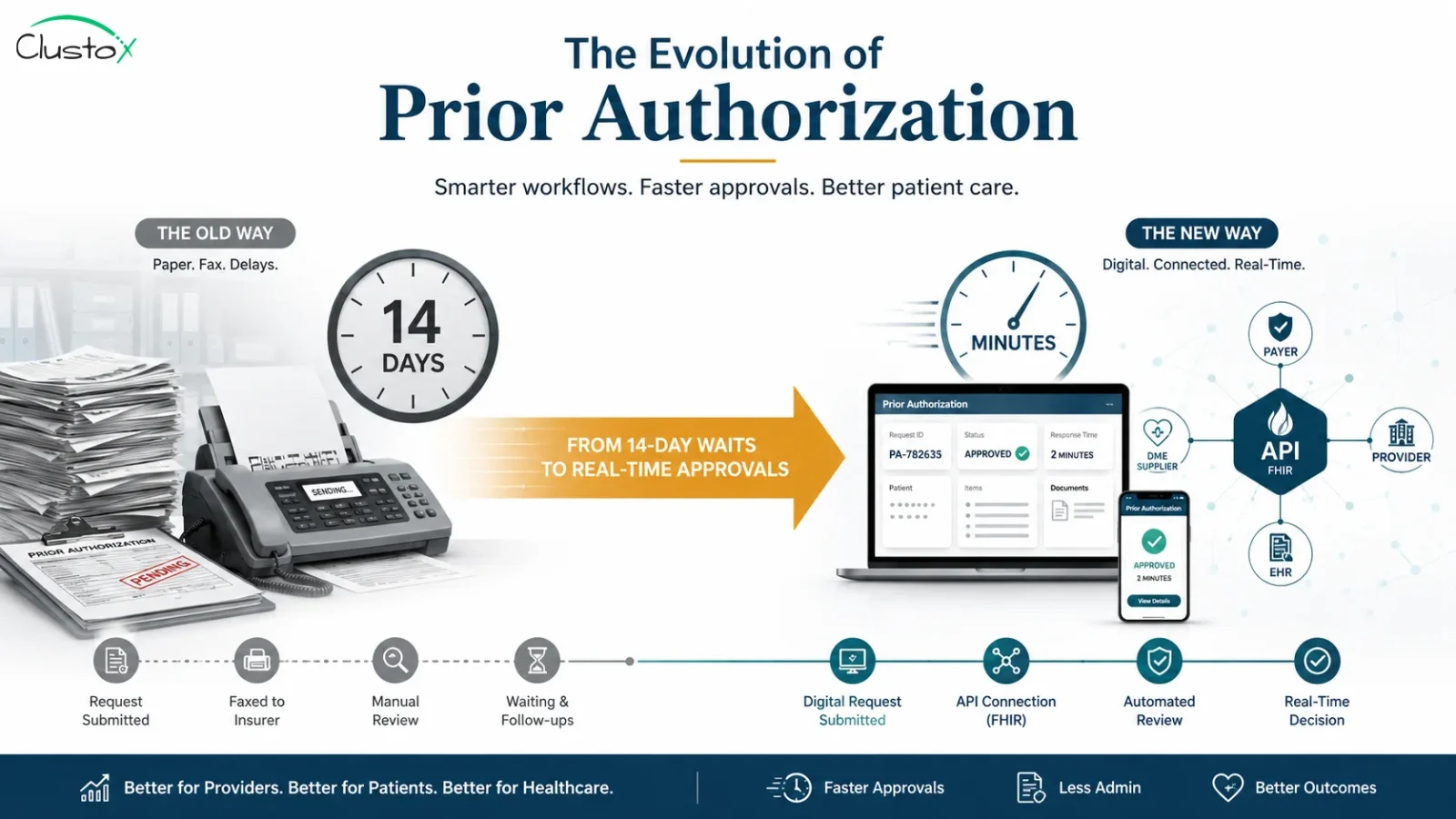
Why Prior Authorization Still Takes Up to 14 Days
The timeline is not an accident. It reflects a process built on faxes, phone calls, and manual review. Each handoff adds time, and each request travels the same slow path.
Most of the delay is not the payer thinking hard about one case. It is the queue, the back-and-forth for missing documents, and the gap between systems that do not talk to each other.
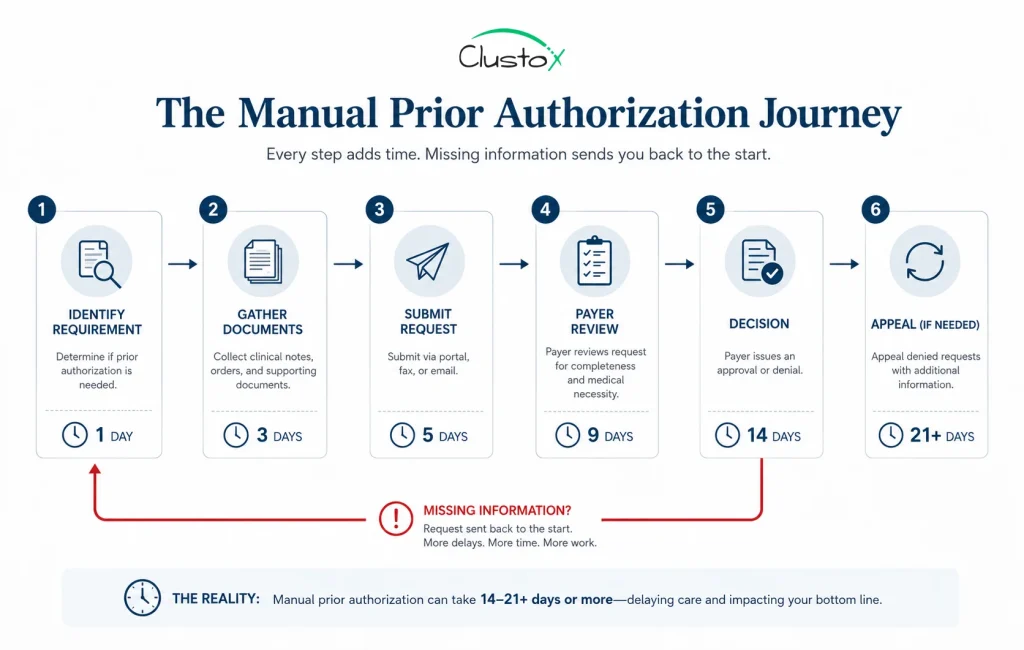
The table below shows what a standard manual prior authorization request looks like, step by step, with the time each stage tends to add.
| Step | What Happens | Typical Time |
|---|---|---|
| Identify the requirement | Staff confirm the item or service needs prior authorization | Hours to 1 day |
| Gather documentation | Pull clinical notes, orders, and supporting records | 1 to 3 days |
| Submit to payer | Send the request by fax, portal, or phone | Same day to 1 day |
| Payer review | A reviewer evaluates medical necessity against coverage rules | Up to 14 days (standard) |
| Decision returned | Approval, denial, or a request for more information | Included above |
| 6. Appeal if denied | Resubmit with added documentation and rationale | Adds days to weeks |
Not every request takes 14 days. Many clear quickly. The real problem is the variability and the manual effort behind each one. A single missing document can reset the clock and turn a routine request into a multi-week chase.
What the CMS Prior Authorization Rule (CMS-0057-F) Changes
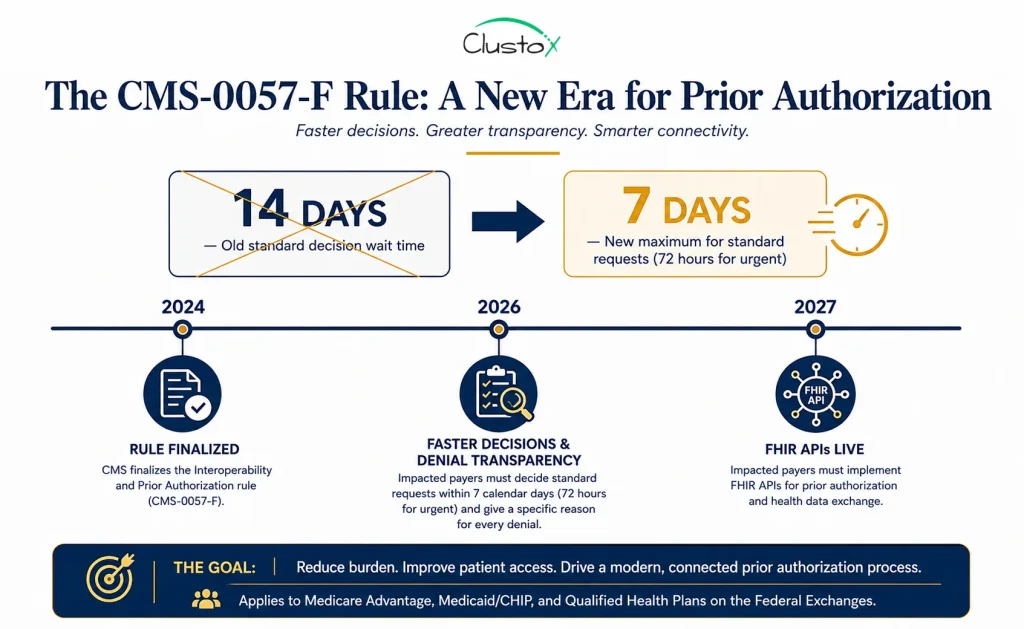
Federal policy is now setting a faster baseline. The CMS Interoperability and Prior Authorization final rule, known as CMS-0057-F, changes both the speed and the transparency of the process for many payers.
CMS finalized the rule in January 2024. It applies to Medicare Advantage plans, state Medicaid and CHIP fee-for-service programs, Medicaid managed care plans, CHIP managed care entities, and qualified health plan issuers on the federal exchanges. Drugs are excluded from the current requirements.
Under the rule, affected payers must return standard prior authorization decisions within 7 calendar days, down from the previous 14, and expedited decisions within 72 hours, according to CMS (2024). That single change cuts the standard ceiling in half.
The rule does more than shorten timelines. The table below summarizes the changes that matter most to operations leaders.
| Change | What It Means for You | Timeline |
|---|---|---|
| Faster decisions | 7 calendar days for standard requests, 72 hours for urgent | Generally January 1, 2026 |
| Denial transparency | Payers must give a specific reason for each denial | Generally January 1, 2026 |
| Public metrics reporting | Payers report prior authorization data publicly each year | Reporting begins in 2026 |
| FHIR-based APIs | Electronic prior authorization plus patient and provider data access | By January 1, 2027 |
One point is worth stating plainly. The rule does not require payers to make decisions in real time. CMS expects some responses to be automated and fast, but many will still need a clinical reviewer. Real-time approval is the direction the policy points, not yet the mandate.
Manual vs. Electronic vs. AI-Assisted Prior Authorization
It helps to see the three ways a prior authorization can move through your operation, side by side. Each is a step up in speed and consistency, and each builds on the one before it.
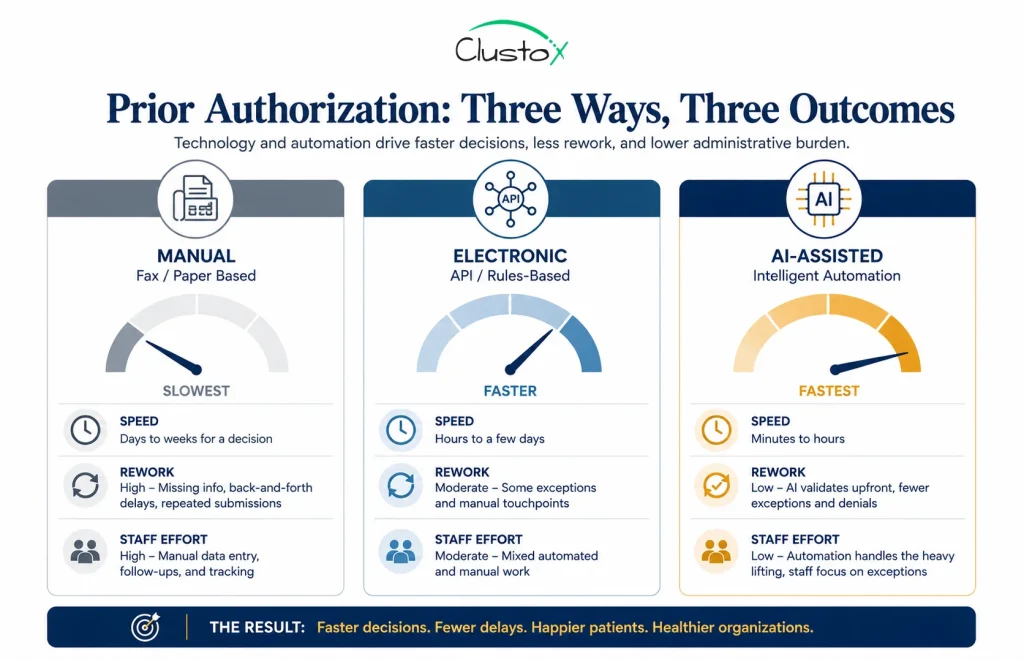
The table below compares them across the dimensions that decide your turnaround and your cost.
| Dimension | Manual | Electronic (ePA) | AI-Assisted |
|---|---|---|---|
| Submission method | Fax, phone, or portal | FHIR-based API | API plus automated drafting |
| Documentation | Staff gather by hand | Staff gather, system sends | System gathers and checks completeness |
| Rule checking | From memory or PDFs | Manual, against the portal | Automated, against coverage criteria |
| Typical turnaround | Up to 14 days | A few days | Hours to 1 to 2 days |
| Rework rate | High | Moderate | Lower, gaps flagged early |
| Staff effort per request | High | Moderate | Low, focused on review |
Electronic prior authorization is the floor the new rule pushes you toward. AI-assisted prior authorization is where the savings compound, because it removes the slow human steps that sit between submission and decision. One point matters here. AI-assisted workflows ride on top of electronic ones, so you need the data plumbing in place first. There is no shortcut around clean, connected inputs.
How Automation and AI Move Prior Authorization Toward Real-Time Approvals
If the rule sets the floor, technology raises the ceiling. Electronic prior authorization and AI are what close the gap between a 7-day rule and a same-day answer.
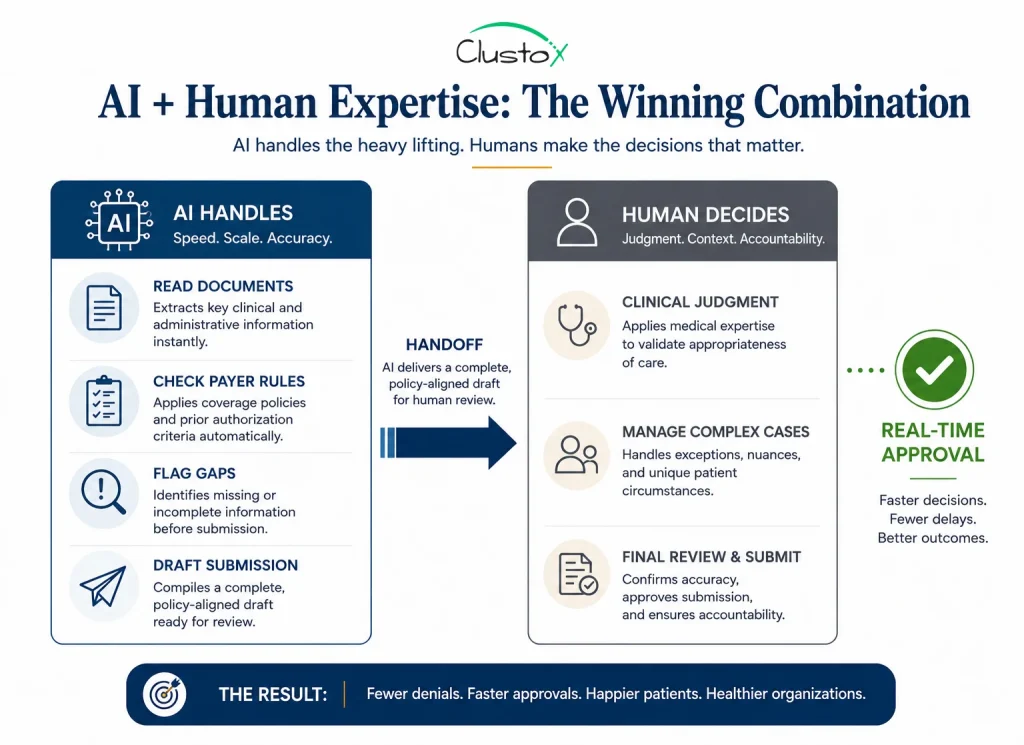
Electronic prior authorization lets your system and the payer system exchange data directly, using the FHIR-based APIs the rule requires. AI then handles the slow human steps. It reads the chart, checks the request against published coverage rules, flags missing documentation before submission, and drafts a clean, complete request the first time.
How an AI Prior Authorization Workflow Works, Step by Step
Under the hood, an AI-assisted workflow usually runs as a short sequence of automated tasks with a human at the end.
Here is the typical order.
- Read the clinical record. The system pulls and reads the chart, the order, and the supporting notes.
- Identify the requirement. It confirms the item or service needs authorization and finds the right payer rule.
- Check against coverage rules. It compares the documentation against the payer’s published coverage criteria.
- Flag what is missing. If something is absent, it surfaces the gap before submission, not after a denial.
- Draft the submission. It assembles a complete, correctly formatted request.
- Route for review. Clear cases proceed automatically, and complex ones go to a human reviewer.
- Track and respond. It monitors status, handles routine follow-ups, and records the outcome.
What Real-Time Prior Authorization Actually Looks Like
In a real-time flow, the request, the supporting documentation, and the payer rule check happen in one connected process. For clear-cut cases that meet published criteria, the system can return an answer in minutes instead of days. The patient leaves with a plan, not a pending status, and your team moves on to the next case.
Where AI Helps, and Where Humans Stay in the Loop
AI is strongest at the repetitive parts. It can read documentation, match it against coverage criteria, identify what is missing, and prepare the submission. That reduces errors and rework, which is where most delay hides.
AI does not replace clinical judgment. Complex or borderline cases still go to a human reviewer, and they should. Honest automation keeps a person in the loop where the decision is not clear and automates the paperwork around that decision. Any vendor who promises a fully human-free process is overselling.
What Faster Prior Authorization Means for Healthcare Operations Leaders
For an owner or COO, this shift is an operations story, not a technology story. Faster approvals change staffing, cash flow, and patient experience at the same time. Get ahead of it, and the new timelines work for you. Wait, and they arrive as pressure.
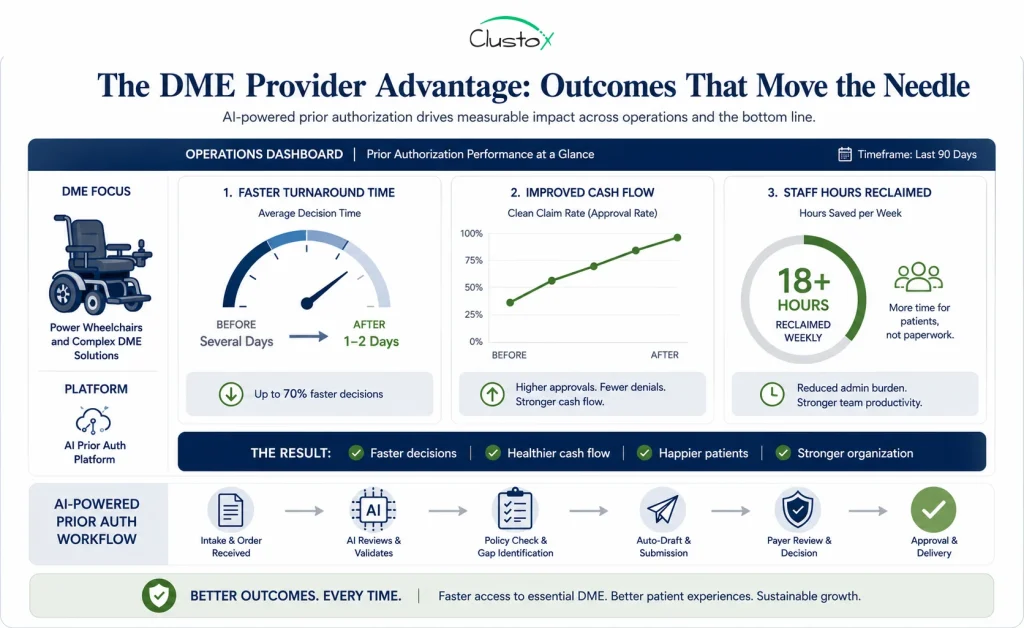
The Impact on Durable Medical Equipment (DME) Providers
The change lands hard in durable medical equipment. Medicare requires prior authorization as a condition of payment for certain DMEPOS items, including many power wheelchairs and some support surfaces. The relevant HCPCS codes are not optional paperwork. Without an affirmed authorization, the claim does not get paid.
That makes a slow authorization a double problem for a DME provider. It is a delayed delivery to a patient who needs equipment, and a delayed payment to a business that has already incurred the cost. Speeding up the authorization step protects both the patient and the balance sheet at once.
The Financial and Staffing Payoff
Faster, cleaner authorizations pay off in three places. Billing moves sooner, so cash arrives sooner. Fewer incomplete submissions mean fewer denials and write-offs. And the staff who once spent their days chasing approvals can move to work that needs a human, such as patient outreach or complex appeals.
In the DME workflows Clustox has built, agentic AI layered on an existing platform such as Brightree has compressed standard prior authorization turnaround from several days to roughly one to two days. Results vary by payer mix and documentation quality, and clinical review still applies. The point is not a single magic number. It is that the slow, manual middle of the process is where the time lives, and it is automatable today.
How to Prepare Your Prior Authorization Workflow: A Practical Roadmap
Preparation is not a single project. It is a sequence. Here is a roadmap you can follow, in order, whatever your starting point. Each step earns the next one.
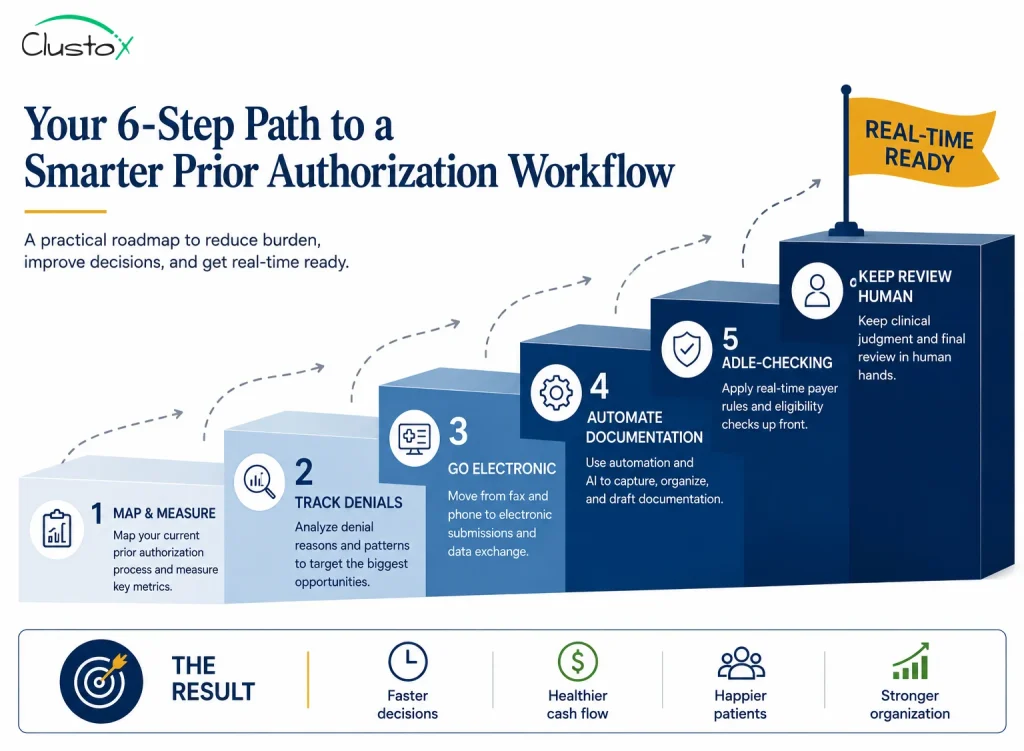
- Map and measure your current workflow. Time each stage and find where requests stall. You cannot fix a queue you have not measured, so this comes first.
- Track and categorize your denials. Group your denials by reason. The new transparency rules give you cleaner data, so use it to find your most common and most fixable rejections.
- Move to electronic prior authorization. Fax and phone will not keep up with a 7-day standard. Connected systems will, and they are the foundation for everything that follows.
- Automate the documentation step first. It is the slowest and most error-prone stage, so it returns the most time when you fix it. Start here before anything fancier.
- Layer in rule-checking and drafting. Once documentation is clean, add the steps that check requests against coverage rules and draft them automatically.
- Keep clinical review human and measure. Automate the paperwork, not the medical decision. Keep a person on the cases that need one, and track turnaround so you can prove the gain.
None of these steps requires a full system replacement. The most reliable path is to add automation on top of the platform you already run, one workflow at a time, and to confirm the result before you scale it.
Common Prior Authorization Mistakes to Avoid
A few predictable mistakes slow teams down or stall their automation efforts. You can sidestep all of them.
- Treating prior authorization as a billing afterthought. It is a front-of-process control, and the earlier you handle it, the fewer surprises appear at billing.
- Automating before you measure. You cannot improve a workflow you have not timed, so map it first.
- Buying a tool before fixing the data. AI needs clean, connected inputs, and a tool on top of messy data will disappoint you.
- Trying to automate clinical judgment. Automate the paperwork, and keep the medical decision with a qualified human.
- Ignoring your denial data. The new transparency rules hand you a roadmap to your biggest problems, so read it.
- Expecting one number to fix everything. Results vary by payer and documentation quality, so set a realistic baseline and improve from there.
Every delayed authorization is a delayed delivery, and a delayed payment.
Clustox combines AI and workflow automation to help DME teams shorten approval times, reduce rework, and reclaim staff hours from manual prior authorization tasks.
Frequently Asked Questions (FAQs)
What Is Electronic Prior Authorization (ePA)?
Electronic prior authorization replaces fax and phone with a direct, system-to-system exchange of data, usually over FHIR-based APIs. It speeds up submission and status checks and reduces manual entry. The CMS-0057-F rule requires affected payers to support these APIs by 2027. It is the foundation that AI-assisted workflows build on.
How Long Does Prior Authorization Take?
It depends on the payer and the request. Standard decisions historically took up to 14 days. Under the CMS-0057-F rule, many payers must now decide standard requests within 7 calendar days and urgent ones within 72 hours. Electronic and AI-assisted workflows can shorten this further for clear-cut cases.
Does the CMS Rule Require Real-Time Prior Authorization?
No. The rule shortens decision timelines and requires electronic prior authorization APIs, but it does not mandate real-time decisions. CMS expects some automated, near-instant responses for straightforward cases. Many requests will still pass through a clinical reviewer.
Will the Faster Rules Apply to All Insurers?
Not all of them. CMS-0057-F covers Medicare Advantage plans, state Medicaid and CHIP programs, Medicaid managed care plans, and Qualified Health Plan issuers on the federal exchanges. Drugs are excluded from the current requirements. Commercial plans outside those categories are not directly bound, though many are moving in the same direction.
Can AI Replace Staff in the Prior Authorization Process?
Not entirely. AI is well suited to reading documentation, checking payer rules, and preparing submissions, which reduces manual work and errors. It does not replace clinical judgment, and complex cases still need human review. The goal is to free your staff for higher-value work, not to remove them.
What Does Prior Authorization Mean for DME Providers Specifically?
Medicare requires prior authorization as a condition of payment for certain DMEPOS items, such as many power wheelchairs and some support surfaces. A slow authorization delays both delivery and payment. Faster, electronic workflows protect your cash flow and get equipment to patients sooner.
How Can My Organization Prepare for Faster Prior Authorization?
Start by mapping your current workflow and timing each step. Move off fax and phone to electronic prior authorization. Automate the documentation-gathering stage first, since it is usually the slowest. Keep clinical review in human hands, and use the new payer reporting data to target your most common denials.
The Bottom Line: Prepare Now, and Faster Approvals Work for You
Prior authorization is moving from a 14-day bottleneck toward a faster, more transparent, and partly automated process. The CMS-0057-F rule sets a 7-day standard for many payers and pushes them onto electronic systems by 2027. Automation and AI carry the process the rest of the way, toward same-day and, for clear cases, near real-time approvals.
For operations leaders, the takeaway is simple. The teams that map their workflow, move to electronic prior authorization, and automate the documentation step will recover hours, protect cash flow, and improve patient experience. The teams that wait will feel the new timelines as pressure instead of relief.
You do not need to fix everything at once. You need to start, in order, with the step that returns the most time.
DISCLAIMER
This guide is written for healthcare operations and technology decision-makers. It is not medical or legal advice. Regulatory references (CMS, HIPAA) are accurate as of the review date, and regulations change. Consult primary sources or qualified counsel for current requirements.