If you run billing operations for a durable medical equipment (DME) supplier, you already know that Medicare prior authorization is not a small administrative task. It is one of the biggest reasons claims get delayed, denied, or sent back for corrections.
In 2026, the rules around Medicare prior authorization for DME have become more specific. CMS has expanded its required authorization list, tightened documentation requirements, and shortened the window for approvals. If your team is still managing this process manually, the margin for error is growing every day.
This guide breaks down exactly what has changed, what you need to do to stay compliant, and how automation tools are helping billing directors and compliance officers reclaim time without adding headcount.
What Is Medicare Prior Authorization for DME, and Why Does It Matter?
Medicare prior authorization is a requirement that a supplier must get approval from CMS before providing certain durable medical equipment to a Medicare beneficiary. Without it, CMS can and will deny payment, even if the equipment is medically necessary.
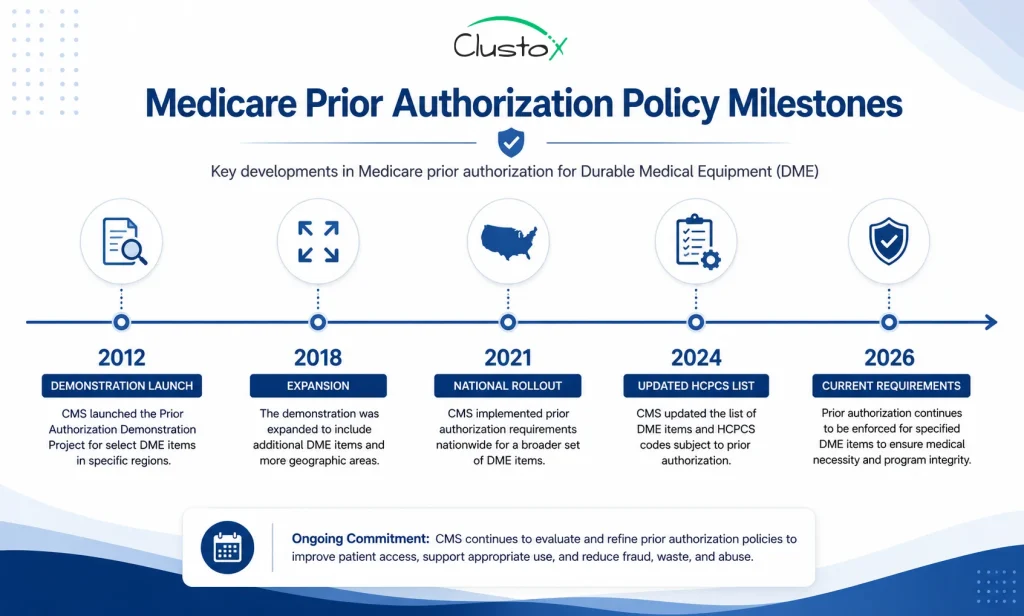
The prior authorization program was first introduced as a demonstration project in 2012. Since then, CMS has expanded it significantly. Today, it applies to a defined list of items that are considered frequently or potentially unnecessary.
For DME suppliers, this means your team has to submit a prior authorization request before the item ships. If the request is missing documentation, uses the wrong HCPCS code, or does not meet the coverage criteria, the request gets denied. You then have to appeal, resubmit, or absorb the loss.
The stakes are high for billing directors because denial rates directly affect cash flow. For compliance officers, incomplete prior auth documentation creates audit exposure. For practice owners and DME business owners, it affects patient care delivery timelines as well.
Table of Contents
Which DME Items Require Medicare Prior Authorization in 2026?
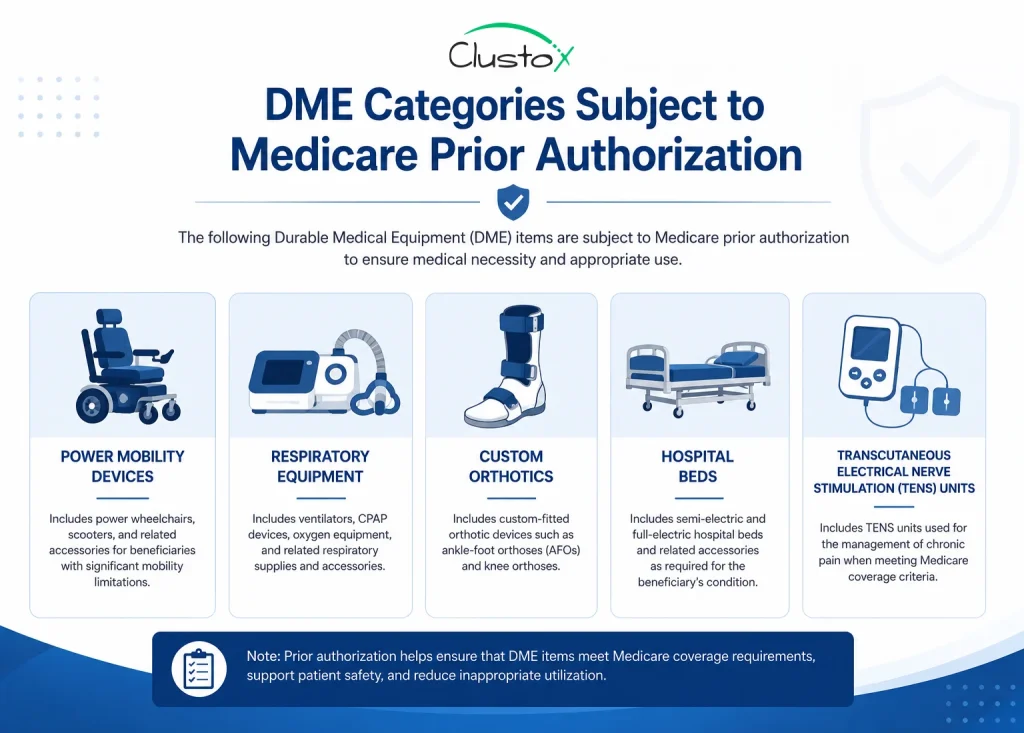
CMS maintains a list of HCPCS codes that require prior authorization as part of its Prior Authorization Program for certain DME, prosthetics, orthotics, and supplies (DMEPOS). In 2026, the following categories are included:
- Power mobility devices (power wheelchairs and scooters)
- Pressure-reducing support surfaces (Group 2 and Group 3 mattresses and overlays)
- Osteogenesis stimulators
- Transcutaneous electrical nerve stimulation (TENS) devices
- Pneumatic compression devices
- Hospital beds (some categories)
- Respiratory assist devices
- Custom fabricated orthotics in certain regions
CMS also has a separate list of items subject to prior authorization in specific geographic areas or under special circumstances. You should check the Medicare Administrative Contractor (MAC) jurisdiction rules that apply to your state, as requirements can vary.
How to Use the Medicare Prior Authorization Search Tool
CMS provides an online Medicare prior authorization search tool at the CMS website. You can use it to look up whether a specific HCPCS code requires prior authorization in your MAC jurisdiction. The tool is updated regularly, so checking it before every new order type is a good habit.
To use it, go to CMS.gov and search for the Prior Authorization and Pre-Claim Review Initiatives page. Enter the HCPCS code and your state, and the tool will return the current authorization status.
What Has Changed with Medicare Prior Authorization Rules in 2026?
The 2026 changes primarily affect three areas: the expanded list of covered items, documentation standards, and processing timelines.
Expanded HCPCS Code List
CMS added new codes to the required prior authorization list starting in 2024 and 2025, with those additions now fully in effect in 2026. Some codes that previously only required prior authorization in demonstration states are now required nationwide. If you have not updated your internal code list recently, there is a real chance you are submitting claims for items that now need upfront approval.
Tighter Documentation Standards
CMS has been clearer about what documentation must accompany a prior authorization request. This includes a detailed physician order with the diagnosis code, length of need, clinical notes supporting medical necessity, and in some cases, proof that conservative treatment was tried first. Missing even one of these elements is enough to trigger a denial.
Shorter Provisional Affirmation Windows
Once CMS issues a prior authorization decision, the provisional affirmation is tied to the order. If the order changes, the patient’s condition changes, or the item is not delivered within the timeframe, you may need to resubmit. In 2026, CMS has reinforced this requirement more strictly.
Real-Time Prior Authorization Pilot Programs
CMS is expanding its real-time prior authorization pilot programs in certain jurisdictions. For suppliers in those areas, the turnaround time expectations are faster, and electronic submission through the FISS or DDE systems is becoming the standard.
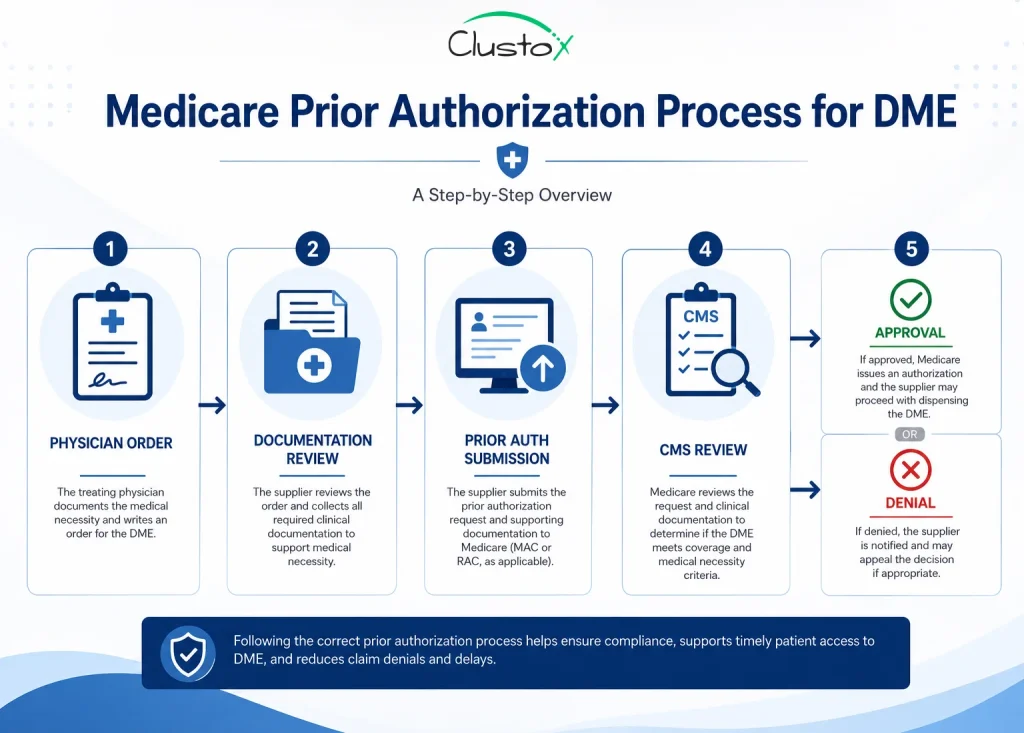
What Does a Complete Medicare Prior Authorization Request Look Like?
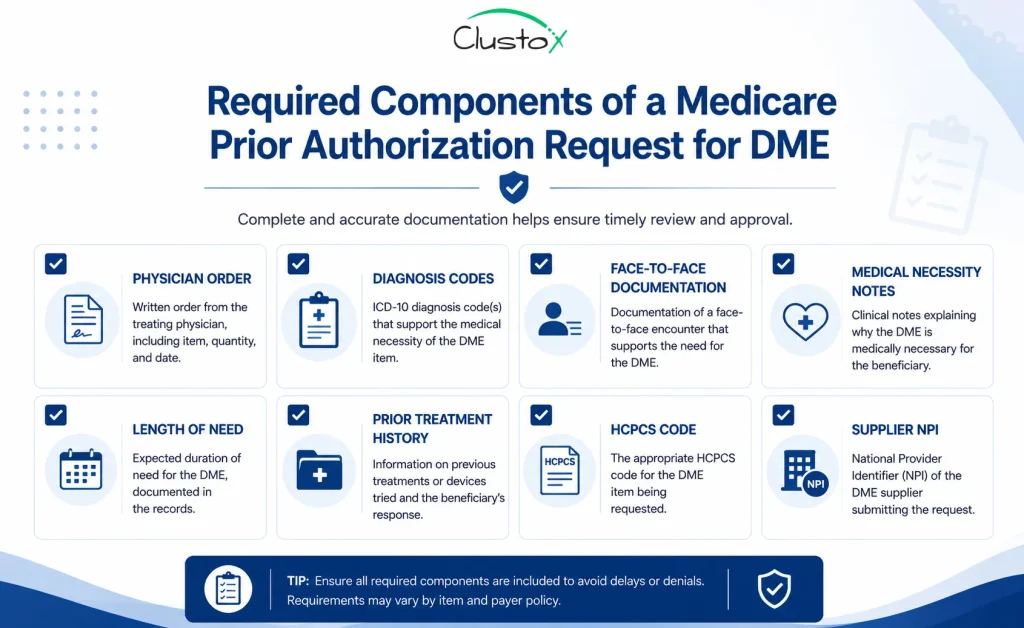
A complete prior authorization request includes more than just the HCPCS code and a note from the physician.
Here is what a well-prepared submission should contain:
| Required Element | Details |
|---|---|
| Detailed Written Order (DWO) | Signed by the treating physician, includes item description, diagnosis, and length of need |
| Face-to-Face Exam Documentation | Clinical notes from an exam within the required timeframe (varies by item) |
| Medical Necessity Documentation | Specific clinical criteria that justify why the item is needed |
| ICD-10 Diagnosis Code(s) | Must align with the item being requested and CMS coverage criteria |
| HCPCS Code | Must be the correct code for the specific item requested |
| Supplier Information | NPI, PTAN, and contact details for the supplier |
| Proof of Prior Conservative Care | Required for some items, such as pressure-reducing support surfaces |
One of the most common reasons prior authorization requests are denied is incomplete or mismatched documentation. The diagnosis code has to support the item. The physician notes have to address the specific LCD (Local Coverage Determination) criteria for that code. Generic notes about the patient’s condition are not enough.
What Happens When a Medicare Prior Authorization Request Is Denied?
A prior authorization denial does not automatically mean the claim is lost. You have options, but each one adds time and cost to the process.
You Can Resubmit with Additional Documentation
If the denial is based on insufficient documentation, you can gather the missing information and resubmit. This is the most common path. However, it delays delivery to the patient and ties up your staff.
You Can Request a Redetermination
If you believe the denial was incorrect, you can request a redetermination from the MAC. This is the first level of the Medicare appeals process. You have 120 days from the date of the denial to submit your redetermination request.
You Can Proceed Without Authorization (at Your Own Risk)
In some cases, you can choose to provide the item without prior authorization and then bill. But if the claim is denied, you will likely not be able to bill the beneficiary unless you have a valid Advance Beneficiary Notice (ABN) on file. This is a high-risk approach that most compliance officers advise against.
How Automation Is Changing the Prior Authorization Process for DME Suppliers
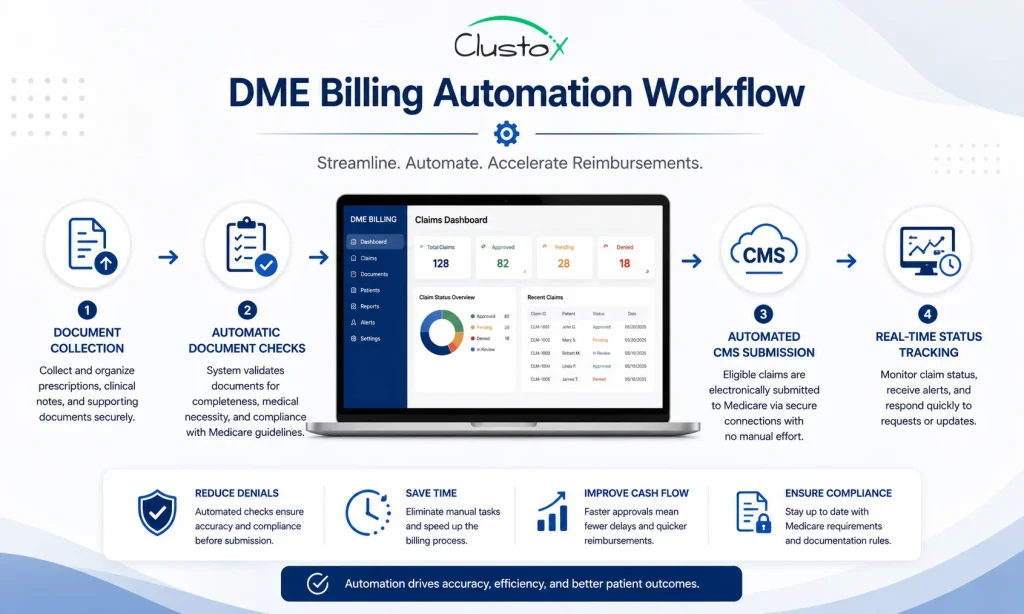
Managing prior authorization manually means your team is doing repetitive tasks that are prone to human error. Checking code lists, reviewing documentation, tracking submission deadlines, and following up on pending approvals all take time. When volume is high, things slip through. Automation tools built specifically for DME billing address this at multiple points in the workflow.
Automated Eligibility and Authorization Checks
Before your team even starts gathering documentation, an automated system can check whether the HCPCS code requires prior authorization for that patient’s specific payer and jurisdiction. This prevents your staff from preparing a submission that was never needed or missing one that was.
Documentation Completeness Checks
Automation tools can scan incoming physician orders and documentation against the CMS criteria for a given code. If something is missing, the system flags it before the submission goes out. This alone can cut first-pass denial rates significantly.
Electronic Submission and Status Tracking
Instead of faxing or manually entering requests into MAC portals, automated systems can submit prior authorization requests electronically and track the status in real time. Your team does not have to call the MAC to find out where a request stands.
Workflow Routing and Alerts
When a prior authorization decision comes back, an automated workflow can route it to the right person, trigger the next step in the order process, or flag it for review if the decision was a denial. Nothing sits in an inbox waiting to be noticed.
Audit Trail and Compliance Reporting
Every submission, approval, denial, and resubmission is logged with a timestamp. This gives compliance officers a clean record for audits and makes it easier to identify patterns in denials that need process changes.
What Should You Look for in a Medicare Prior Authorization Automation Tool?
Not all automation tools are built with DME billing in mind. If you are evaluating options, here are the capabilities that matter most:
- Integration with CMS systems: The tool should connect directly to the FISS system or your MAC’s portal for electronic submission.
- HCPCS and LCD coverage: The tool should have a current, maintained database of codes that require prior authorization and the LCD criteria associated with each.
- Documentation review: Look for tools that check documentation against CMS requirements before submission, not just after a denial.
- Denial management: The tool should flag denials, categorize them by reason code, and help you route them to the right resolution path.
- EHR and billing system integration: If the tool does not connect to your existing systems, it will create more manual work, not less.
- Reporting and analytics: You need visibility into your authorization approval rates, denial trends, and average turnaround times.
Some platforms offer prior authorization as one feature within a broader DME billing suite. Others specialize in authorization management specifically. The right fit depends on where your current process is breaking down.
How to Build an Internal Compliance Process Around Prior Authorization
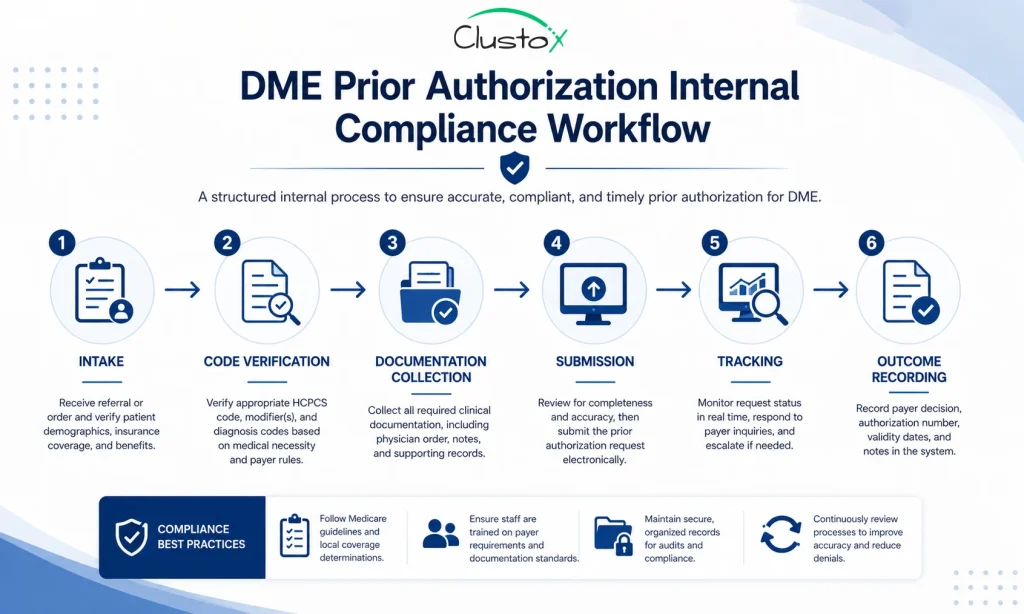
Automation is a force multiplier, but it works best when your internal process is structured. Here is how to build a prior authorization compliance framework that holds up under audit and supports your billing team.
Step 1: Maintain a Current Code List
Assign someone on your team to review the CMS Prior Authorization Program updates every quarter. CMS updates the required HCPCS code list, and your internal documentation needs to reflect those changes. A stale code list is a liability.
Step 2: Create Item-Specific Documentation Checklists
For each high-volume item that requires prior authorization, build a documentation checklist based on the applicable LCD. Your team should not have to guess what is required. A clear checklist reduces errors and speeds up the intake process.
Step 3: Set Submission Deadlines
Prior authorization has to happen before the item ships. Build a submission deadline into your order workflow. If a prior auth request is not submitted within a defined window after the order is received, someone should be notified.
Step 4: Track and Categorize Denials
Every denial should be logged, categorized by reason code, and reviewed. If the same code is getting denied repeatedly for the same reason, that is a process problem, not a one-off error. Monthly denial reviews help you catch these patterns early.
Step 5: Document Everything
In the event of a CMS audit, you need to show that your prior authorization process was followed correctly. Keep records of every submission, every approval, and every denial. Include the date of submission, the decision, and any follow-up actions taken.
Common Medicare Prior Authorization Denial Reasons and How to Fix Them
| Denial Reason | What It Means | How to Fix It |
|---|---|---|
| Insufficient documentation | The clinical notes do not meet LCD criteria | Review the LCD and resubmit with specific supporting documentation |
| Wrong HCPCS code | The code submitted does not match the item or does not require PA | Verify the correct code using the CMS search tool and resubmit |
| Missing physician signature | The DWO is unsigned or signed outside the required timeframe | Get a new signed order and resubmit |
| No proof of conservative care | For some items, you must show that less intensive options were tried | Include clinical notes documenting prior treatment attempts |
| Order outside coverage criteria | The patient's diagnosis does not support the item under Medicare policy | Review the LCD coverage criteria and consult with the referring physician |
Conclusion
Medicare prior authorization for DME is not going to get simpler. CMS continues to expand the list of items that require upfront approval, and the documentation standards are getting more specific every year.
If you are a billing director, compliance officer, or DME business owner, the question is not whether prior authorization affects your operations. It clearly does. The question is whether your current process is built to handle it at scale without burning out your staff or leaving money on the table.
The suppliers who are managing this well in 2026 are not doing it with more people. They are doing it with better processes and the right automation tools. That means checking every code before submission, catching documentation gaps early, submitting electronically, and tracking outcomes so you can improve over time.
Start with an audit of your current denial rate for prior authorization. If it is higher than 10 percent, that is where your process needs work. If your team is spending significant time on phone calls to check authorization status, that is time that automation can give back.
Getting prior authorization right is not just a compliance issue. It is a business issue, and in 2026, the tools exist to handle it far more efficiently than most DME suppliers currently are.
Frequently Asked Questions
How do I search for which DME items require Medicare prior authorization?
CMS provides a prior authorization search tool on its website where you can enter a HCPCS code and your state to check the current requirements. You can also check with your Medicare Administrative Contractor (MAC) for jurisdiction-specific guidance. It is a good idea to check before submitting any new order type.
What happens if I provide DME without getting prior authorization first?
If you provide an item that requires prior authorization without getting one, Medicare will almost certainly deny the claim. You generally cannot bill the beneficiary unless you have a valid Advance Beneficiary Notice on file. This creates a financial loss for your business and potential compliance exposure.
How long does Medicare prior authorization take?
CMS is required to respond to standard prior authorization requests within 10 business days and expedited requests within 2 business days when there is a medical urgency. Response times can vary depending on the MAC and the completeness of your submission. Incomplete submissions often cause delays.
Can I automate the Medicare prior authorization process?
Yes, several DME billing platforms offer automation features that handle eligibility checks, documentation review, electronic submission, and status tracking. Automation reduces manual errors and speeds up the approval process. It is especially valuable for high-volume suppliers managing multiple item types.
What documentation is required for a Medicare prior authorization request?
You typically need a detailed written order from the treating physician, clinical notes supporting medical necessity, the appropriate ICD-10 and HCPCS codes, and in some cases, documentation of prior conservative treatment. The exact requirements depend on the item and the applicable local coverage determination.
How do I appeal a Medicare prior authorization denial?
If your prior authorization request is denied, you can resubmit with additional documentation or request a redetermination from the MAC. A redetermination is the first level of the Medicare appeals process, and you have 120 days from the denial date to file. Tracking your denial reasons carefully helps you build a stronger resubmission.
Too Many Medicare Prior Authorization Denials?
Improve DME prior authorization accuracy with automated workflows that help prevent avoidable denials and missing documentation.