
Quick Answer
Most prior authorization companies promise faster approvals. Very few deliver them consistently in a DME environment. This guide gives you a practical evaluation framework: the criteria that separate capable vendors from expensive experiments, the red flags that show up too late after you have already signed, and the questions you should be asking before you commit.
If you run billing or revenue cycle operations at a DME supplier, you already know what a bad prior authorization process costs you. Claims sit. Staff make follow-up calls that go nowhere. Auth requests get denied on documentation technicalities that a better system would have caught on day one. Cash flow slows while your team burns time on manual work that should not require a human at all.
The market for prior authorization companies has grown significantly over the past few years. Vendors now range from basic software portals that digitize fax submissions to fully managed services and AI-powered workflow engines that handle the entire authorization loop. That range is good for buyers in theory. In practice, it means you have to do real due diligence to avoid paying a premium for a tool that is barely better than what you already have.
This guide is written specifically for DME operations. The evaluation criteria here reflect the realities of durable medical equipment billing: CMS compliance requirements, payer-specific documentation rules, HCPCS coding complexity, and the need to integrate with platforms like Brightree, NikoHealth, and TIMS.
If you are a Director of Billing, an Owner, or a CFO making this vendor decision in 2026, this is the framework you need.
What Do Prior Authorization Companies Actually Do for DME Suppliers?
Prior authorization companies exist to sit between your team and the payer and handle the documentation, submission, follow-up, and tracking that the auth process requires. In DME, that process is more complex than in most other healthcare verticals.
A standard DME prior auth workflow involves confirming patient eligibility, gathering the Letter of Medical Necessity (LMN) and supporting clinical documentation, matching everything to the correct HCPCS codes and payer-specific coverage criteria, submitting through the payer’s required channel (fax, portal, or EDI), tracking status, responding to requests for additional information, and logging the outcome against the order. For high-ticket items like power wheelchairs, respiratory equipment, or custom orthotics, a single authorization can require 10 to 20 documents.
Table of Contents
Prior authorization companies handle some or all of that workflow, depending on their model.
There are three primary models in the market today.
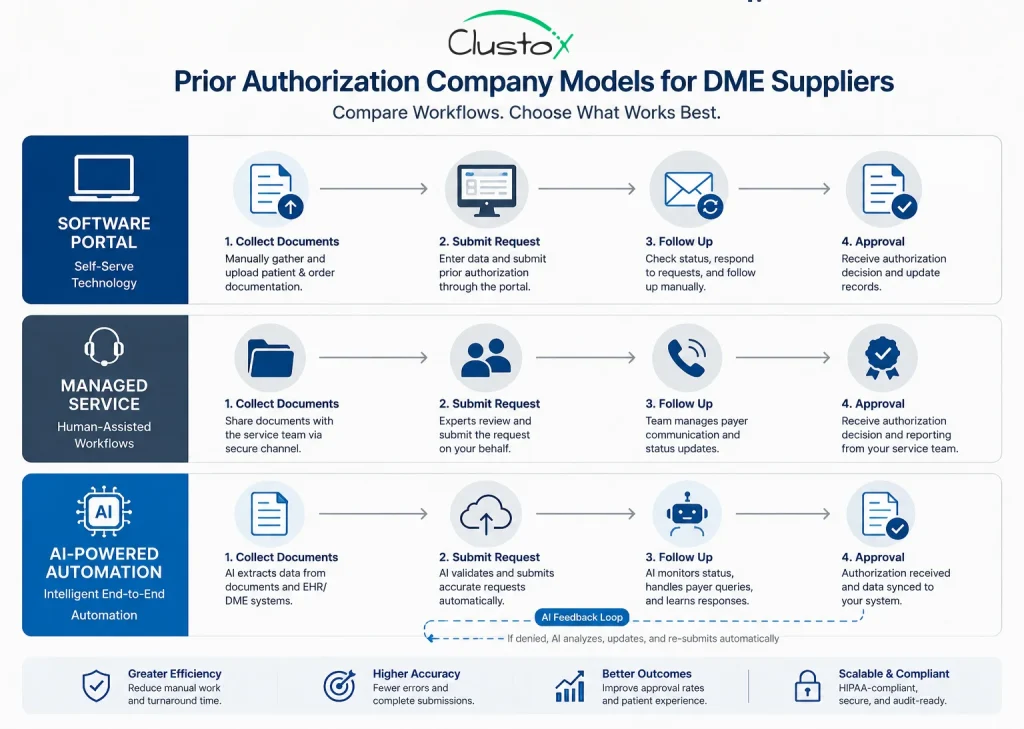
| Model | What It Covers | Best For |
|---|---|---|
| Software portal only | Digital submission and status tracking. Your team still prepares documents and manages follow-up. | Suppliers with strong internal staff who want a better submission interface. |
| Managed service | A vendor team handles submission, follow-up, and denial response on your behalf. | Suppliers with high volume and limited internal bandwidth. |
| AI-powered automation | Automated document collection, compliance checks, submission, and status monitoring. Human review for exceptions. | Suppliers who want to scale without adding headcount and who are integrating with modern DME software. |
Understanding which model a vendor operates under is the first thing to establish. Many companies market themselves as AI-powered but are operating a managed service with software tools layered on top. The distinction matters because it affects pricing, turnaround times, scalability, and what happens when volume spikes.
Why DME Requires Specialized Prior Authorization Vendors
Not every prior authorization company is built for DME. Many are designed for physician practices or hospitals, where the auth workflow is simpler and the payer mix is more predictable. If you bring one of those vendors into a DME environment, you will run into gaps quickly.
Here is what makes DME authorization different from general medical prior auth.
HCPCS code complexity
DME billing runs on HCPCS Level II codes, not CPT codes. A vendor whose compliance engine is built around CPT workflows will not catch payer-specific documentation requirements tied to HCPCS L codes, E codes, or K codes. That creates documentation gaps that result in denials.
CMS coverage determination requirements
Medicare DME prior auth for certain items, including power mobility devices and certain respiratory equipment, follows Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs) issued by CMS.
A vendor who does not have those requirements mapped into their documentation checklist is going to miss criteria that lead to denial.
LMN documentation standards
The Letter of Medical Necessity is the cornerstone of most DME auth requests. Payers have specific requirements for what an LMN must contain, and those requirements vary by payer and by product category. A generalist vendor may not have those requirements built into their intake workflow.
Strong documentation workflows should account for both LMNs and the Certificate of Medical Necessity, especially for high-scrutiny product categories where incomplete clinical justification can slow approvals or increase denial risk.
Payer-specific portal requirements
Medicare Advantage plans, commercial insurers, and Medicaid managed care organizations each have their own submission portals and documentation standards. A vendor who handles DME volume will have these mapped. A vendor who does not will rely on your staff to fill the gap.
Integration with DME-specific software
Your auth vendor needs to work with your operations software. If you are running Brightree, NikoHealth, TIMS, or another DME platform, the prior auth workflow needs to connect to order management, patient records, and billing. A vendor who requires manual data entry between systems adds cost and error risk.
Unlike general medical billing workflows, prior authorization for DME involves product-specific documentation rules, HCPCS verification, LMN requirements, and payer-specific submission pathways that vary across respiratory equipment, mobility devices, and sleep therapy products.
What Criteria Should You Use to Evaluate Prior Authorization Companies?
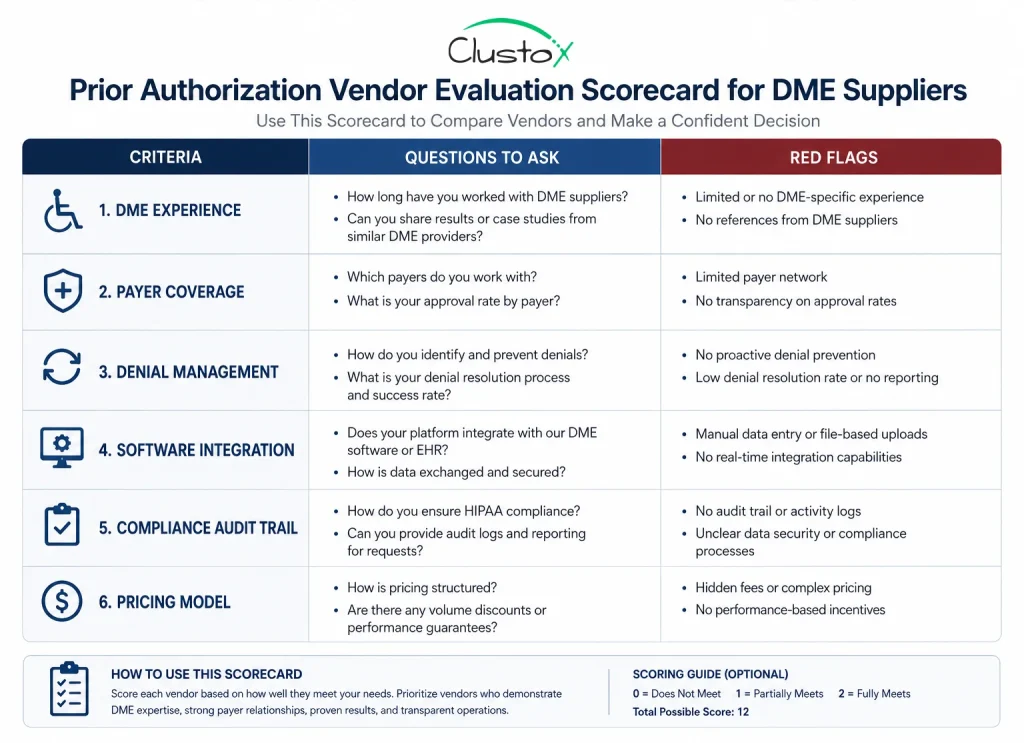
When you get past the vendor marketing and into an actual evaluation, these are the criteria that matter for a DME operation.
1. DME-specific authorization experience
Ask the vendor for their book of business. What percentage of their clients are DME suppliers? What product categories do they handle auth for? If they do not have meaningful DME experience, they are learning on your dime. That is a risk you do not have to take when specialized vendors exist.
The right follow-up question: ask for denial rates by product category. A vendor who handles power mobility auth at scale should be able to tell you their approval rate on first submission. If they cannot give you that number, they are not tracking it closely enough.
2. Payer coverage and turnaround SLAs
“Coverage” means the list of payers the vendor can submit to and the channels they use (direct portal access, clearinghouse, phone, and fax). “Turnaround time” means how long from order to auth decision. These are two different metrics that vendors sometimes conflate.
3. Denial management workflow
Denials are not just a prior auth failure. They are also a revenue recovery opportunity if you have a vendor who can identify the denial reason, correct the documentation, and resubmit quickly. Ask specifically about how the vendor handles initial denials. Do they have a clinical review step? Do they track denial reasons and feed that data back into their intake process to prevent recurrence?
A vendor whose denial workflow is “we flag it and send it back to you” is not a denial management service. It is a submission service with a notify-and-exit process.
4. Integration with your DME software stack
This is not a nice-to-have. If the vendor requires your team to rekey patient data, order information, or clinical documentation into their platform, you are adding labor cost and a source of transcription errors. Ask for a live integration demo with your specific platform. Brightree has an open API that a competent vendor should be able to connect to. The same applies to NikoHealth and TIMS.
Also ask what happens when integration breaks. Who is responsible for the fix? What is the SLA for restoring data flow?
5. Compliance and audit trail
CMS and payer audits happen. When they do, you need documentation that shows the authorization process was executed correctly: what was submitted, when it was submitted, what the payer response was, and what follow-up actions were taken. A vendor whose platform does not produce a clean audit trail is a liability.
Any vendor handling protected health information should be able to explain its audit trails, user access controls, encryption standards, and HIPAA technical safeguards before touching authorization workflows tied to patient documentation and payer communication.
Ask to see a sample audit report. If the vendor cannot produce one, that is a gap worth noting.
6. Pricing model and volume economics
Prior authorization companies typically price on one of three models: a per-authorization fee, monthly subscription, or a percentage of recovered revenue. For DME operations, the per-auth model is usually most transparent because it scales directly with volume. The percentage model can look attractive but may create misaligned incentives on complex auths where the approval value is high.
Get a clear answer on what is included in the base price and what triggers additional charges. Common add-ons include denial appeals, expedited processing, and portal access fees for certain payer networks.
What Red Flags Should You Watch for During a Vendor Demo?
Vendor demos are designed to show you the best-case scenario. Here are the signals that tell you more about how the product performs under real DME conditions.
- They demo with generic healthcare scenarios, not DME-specific workflows. Ask them to walk through a power wheelchair authorization or a home oxygen authorization. If they cannot do it fluently, they are not specialists.
- They cannot show you a real integration with your software. A slide deck showing a logo connection is not the same as a live API sync. Push for a live demo in a sandbox environment.
- Turnaround time guarantees have no contractual basis. If a vendor promises 48-hour auths but the SLA in the contract says “commercially reasonable efforts,” those are two different things.
- They do not track first-pass approval rates. This is the core metric for prior auth quality. If a vendor does not track it or will not share it, that tells you something about how they think about performance.
- The escalation path is unclear. Ask what happens when a case requires clinical review or when a payer rejects documentation. Who handles it? What is the timeline? Vague answers here create operational risk.
- References are only from non-DME customers. A vendor with strong hospital or physician practice references is not automatically qualified for DME. Ask specifically for DME supplier references, ideally in your product category and volume range.
How Does AI Change the Prior Authorization Landscape for DME?
AI is having a real effect on prior authorization workflows, but the impact varies significantly depending on how a vendor has implemented it. The hype significantly outpaces the reality in a number of cases, so it is worth being specific about what AI can and cannot do in this context.
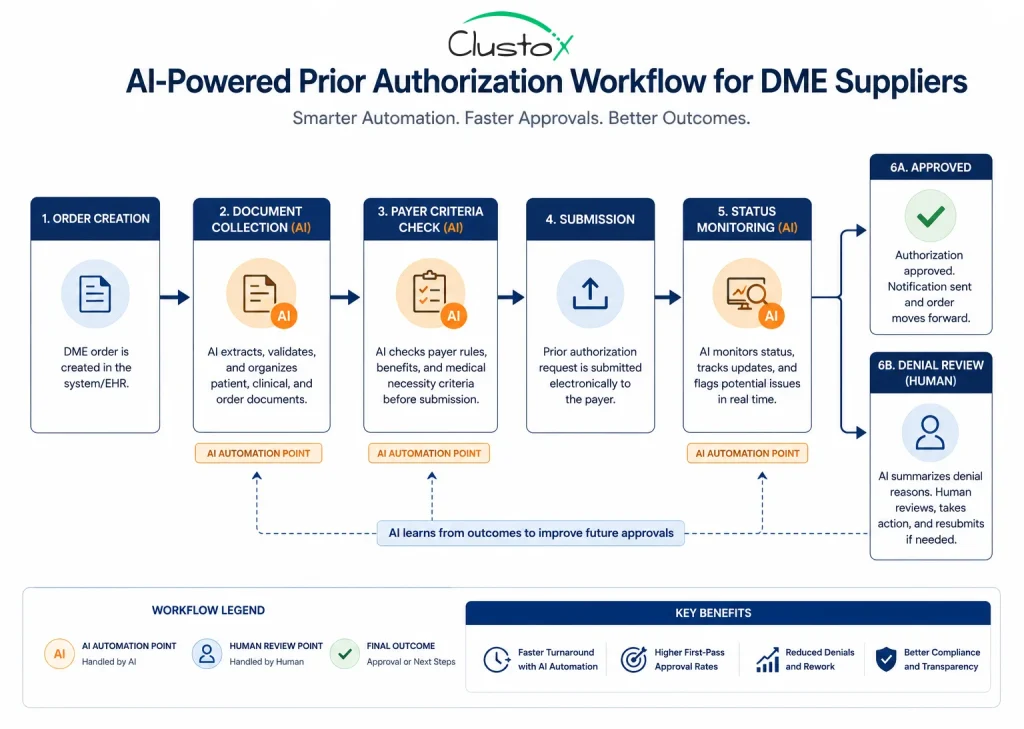
Where AI adds genuine value
Document completeness checking is one of the clearest AI use cases in DME prior auth. An AI system that can ingest a clinical note, an LMN, and an order, then check them against payer-specific coverage criteria before submission, catches errors that humans miss under time pressure. That translates directly to higher first-pass approval rates and fewer back-and-forth cycles with clinical staff.
Status monitoring is another. An AI layer that continuously checks payer portals for authorization status, flags pending requests that are approaching payer decision deadlines, and sends alerts before expirations requires no human time once it is configured correctly.
Denial pattern analysis is a longer-term value driver. A system that tracks why specific request types get denied, by payer and by product category, can surface process improvements that a human reviewer working on individual cases would never see across the full volume.
Modern authorization workflows are moving beyond static automation tools toward agentic AI systems that can coordinate documentation checks, payer routing, escalation logic, and follow-up workflows across multiple operational steps instead of relying on isolated rule-based triggers.
Where AI does not replace judgment
AI does not replace clinical knowledge when a payer pushes back on medical necessity grounds. It does not replace the relationship a managed service team may have with a payer’s utilization management department. And it does not replace experienced human review when a case is genuinely complex.
A reliable AI-powered prior auth vendor will tell you exactly where the system automates and where a human takes over. Be skeptical of any vendor who claims full automation without exceptions.
Prior Authorization Company Comparison: Key Vendor Evaluation Factors
Use this framework when you are comparing vendors side by side.
Fill in your findings from demos, references, and contract review.
| Evaluation Factor | Weight | What to Look For | Deal-Breaker Threshold |
|---|---|---|---|
| DME-specific experience | High | Percentage of book in DME named product categories | Less than 30% DME clients |
| First-pass approval rate | High | Vendor-reported rate by product category | Below 80% on standard items |
| Payer network coverage | High | Full list of payers; portal vs. manual submission | Missing your top 5 payers |
| Brightree / NikoHealth / TIMS integration | High | Live API demo; documented sync frequency | Manual data entry required |
| Denial management workflow | Medium | Clinical review step; resubmission SLA; pattern tracking | No clinical review capability |
| Audit trail and reporting | Medium | Sample report; exportable documentation log | No exportable audit log |
| Turnaround SLA (contractual) | Medium | Days to decision, contractually committed | SLA absent from contract |
| Pricing transparency | Medium | Clear per-auth or subscription pricing; add-on fee list | Percentage of recovery with no cap |
What Does Good Vendor Onboarding Look Like?
How a prior authorization company handles your onboarding tells you a great deal about how they will operate once you are live. A vendor who rushes you through setup to get to billing is a vendor whose implementation process is under-resourced.
A well-structured onboarding for a DME prior authorization vendor should include at minimum: a configuration session where payer-specific rules and documentation requirements are mapped to your product mix; an integration test in a staging environment before any live patient data is touched; a training session for your billing and clinical documentation team that covers their role in the new workflow; and a defined go-live plan with a parallel period where the old and new processes run simultaneously.
The parallel period is important. It gives you a baseline to measure the vendor’s performance against your current process. If the vendor pushes back on running a parallel period, ask why.
What Questions Should You Ask References Before Signing?
References from a vendor’s existing DME clients are one of the most reliable inputs you have. Here are the questions worth asking.
- What is your actual first-pass approval rate since going live with this vendor, and how does it compare to what you were running before?
- How does the vendor handle denials? Do they have a clinical team that reviews and resubmits, or do they send it back to your staff?
- How long did integration with your software take, and were there issues during the process?
- What does escalation look like when a case is complex or a payer is unresponsive?
- Has the vendor’s pricing changed since you signed? Were there fees you did not expect?
- If you had to do it over, what would you negotiate differently in the contract?
Frequently Asked Questions (FAQs)
How long does prior authorization typically take in DME?
Standard prior auth decisions from major payers can range from 24 hours for straightforward items with clean documentation to 10 or more business days for complex equipment like custom orthotics or power mobility devices. A well-run prior auth vendor with strong payer relationships and complete documentation on first submission should be able to achieve two to four business days on most standard items. Medicare Advantage and commercial payers vary significantly.
What is a first-pass approval rate, and what should you expect?
The first-pass approval rate is the percentage of authorization requests that are approved without requiring any resubmission, additional documentation, or appeal. A higher first-pass rate means your auth is cleaner, your revenue cycle is faster, and your staff spends less time in denial management loops.
For a vendor with strong DME experience and a well-configured documentation check process, you should expect first-pass rates above 80% on standard covered items. Below that number on routine authorizations is a flag worth investigating.
Can prior authorization companies integrate with Brightree or NikoHealth?
The leading specialized DME prior auth vendors have integration capabilities with Brightree, NikoHealth, and TIMS. The depth of that integration varies. At minimum, you want bidirectional data flow so that order data from your DME platform populates the auth request automatically and the auth status updates back into the order record without manual entry.
How is AI being used in prior authorization for DME in 2026?
The most practical AI applications in DME prior auth right now are document completeness checking before submission, automated payer portal status monitoring, and denial pattern analysis at scale. Some vendors are using AI to draft initial auth requests from structured order data, which reduces the documentation burden on your clinical and billing staff.
The Bottom Line
The right prior authorization company for your DME operation is not necessarily the biggest name in the market or the vendor with the most polished demo. It is the one who has done this work in DME before, who can connect to your software without requiring your team to manually bridge the gap, who tracks first-pass approval rates and will show you theirs, and who has a clear denial management workflow backed by clinical review capability.
The evaluation process takes time up front. That time is worth it. Switching prior auth vendors after a bad implementation is expensive in both money and operational disruption. Getting it right on the first selection protects your revenue cycle and your team’s capacity.
Use the criteria and questions in this guide as your starting framework. Add to them based on your specific payer mix, product categories, and software environment. And if you are considering AI-powered automation as part of this decision, be specific about what the vendor means by AI, where human review starts, and what your SLA looks like when the automated process needs escalation.
Your prior auth process is a direct line to cash flow. Treat the vendor decision accordingly.
Still losing hours to manual prior authorization follow-ups and payer delays?
Clustox helps DME suppliers automate prior auth workflows with AI systems designed around real payer requirements, documentation logic, and DME software integrations.
Disclaimer
This article is intended for DME providers, operations leaders, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, accreditation standards) are accurate as of the review date; regulations change frequently, and providers should consult primary sources or qualified counsel for current requirements.