Electronic prior authorization, or ePA, is the electronic exchange of prior authorization requests, supporting documents, status updates, and decisions between providers, suppliers, and payers.
For DME teams, the point is simple: fewer status calls, fewer duplicate uploads, and a cleaner record of what was sent, when it was sent, and what the payer asked for next.
In 2026, ePA is real, but it is not uniform. CMS operational requirements for certain impacted payers started on January 1, 2026, while many of the API build requirements under CMS-0057-F landed primarily on January 1, 2027. That means DME operators still live in a mixed environment of APIs, payer portals, clearinghouse workflows, and fax fallbacks.
The practical question is not whether ePA matters. It is where it is mature enough to reduce work today, where it still needs human review, and how an AI-first workflow can close the gaps without creating compliance problems.
What Does “Electronic Prior Authorization” Mean in DME?
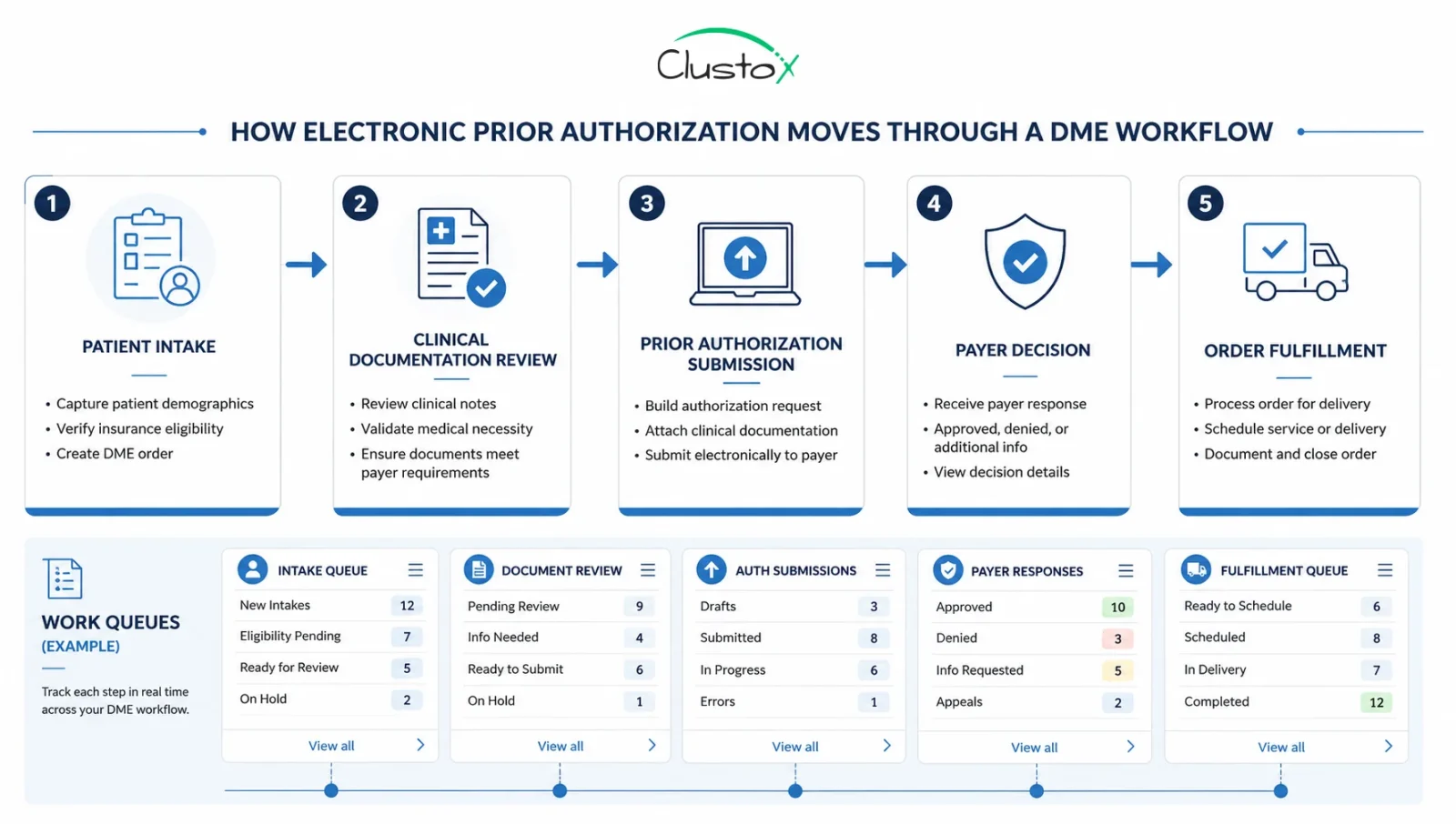
For DME, ePA usually covers the digital handling of medical-necessity review for items such as equipment, supplies, and related services billed under a medical benefit. In an ideal flow, the supplier or ordering provider sends the authorization request electronically, the payer returns the status electronically, and any request for more information is tracked in the same workflow.
That is different from a simple portal upload. A portal can still be electronic, but it often behaves like a manual inbox. True ePA is closer to a structured transaction, or at least a structured API workflow, where systems can exchange data and keep status synchronized.
This distinction matters for DME leaders because the hidden cost in prior authorization is not only the initial submission. It is the follow-up work: missing attachments, unclear denial reasons, duplicate entries in a practice management system, and handoffs between the billing, intake, and documentation teams.
Table of Contents
The Standards Behind ePA?
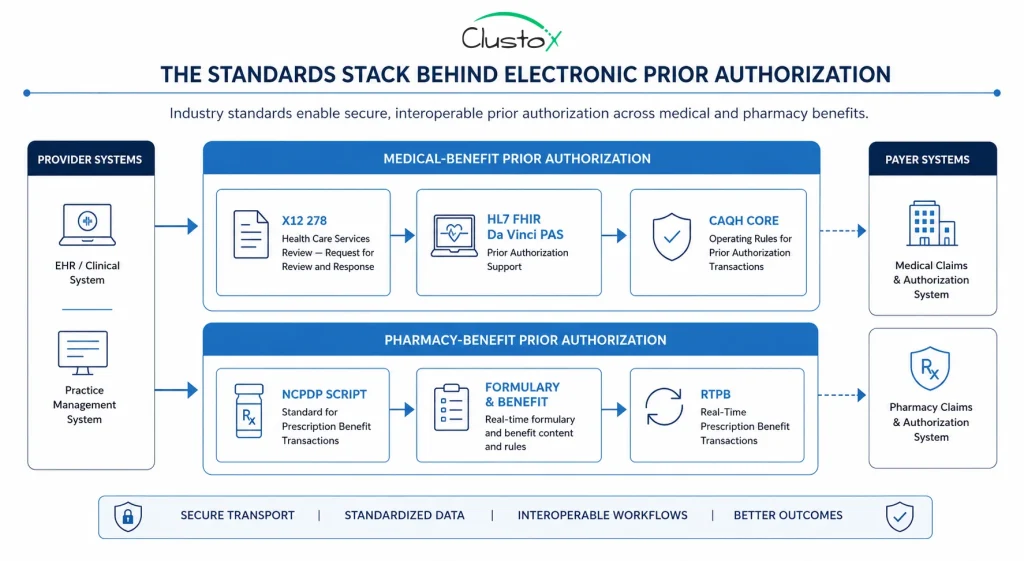
The standards stack is where many teams get lost. In DME, the safest way to explain it is to separate medical-benefit prior authorization from pharmacy-benefit prior authorization.
| Standard | Where it fits | What DME teams should know |
|---|---|---|
| X12 278 | HIPAA transaction standard for health care services review information | Still, the legacy standard to know for medical prior authorization. Many trading partners and clearinghouse workflows are built around it. |
| HL7 FHIR Da Vinci PAS | FHIR implementation guide for prior authorization support | This is the direction CMS encourages for API-based ePA. It helps systems exchange request, response, and supporting status data in a more modern way. |
| CAQH CORE prior authorization and referrals operating rules | Rules that standardize how prior auth transactions, attachments, and portal workflows should behave | Useful when you need fewer hand-built exceptions across trading partners. It helps make electronic exchanges more predictable. |
| NCPDP SCRIPT | Pharmacy-benefit ePA and e-prescribing transactions | Important when the authorization sits under a pharmacy workflow or Part D context. It is not the main standard for most medical-benefit DME prior authorization. |
CMS says impacted payers must implement a Prior Authorization API that can show covered items and services, identify documentation requirements, support request and response exchange, and return approvals; denials with a specific reason; or requests for more information.
CMS also encouraged the use of the HL7 Da Vinci PAS implementation guide in the 2024 final rule.
NCPDP belongs in this article because many operators hear the term “ePA” and assume one standard handles every case. It does not. CMS still treats drugs and non-drug medical items differently in 2026.
The 2024 final rule focused on non-drug items and services, while the 2026 proposed rule addresses drugs and names NCPDP SCRIPT, Formulary, and Benefit, and Real-Time Prescription Benefit standards for that path.
Payer Support for ePA in 2026
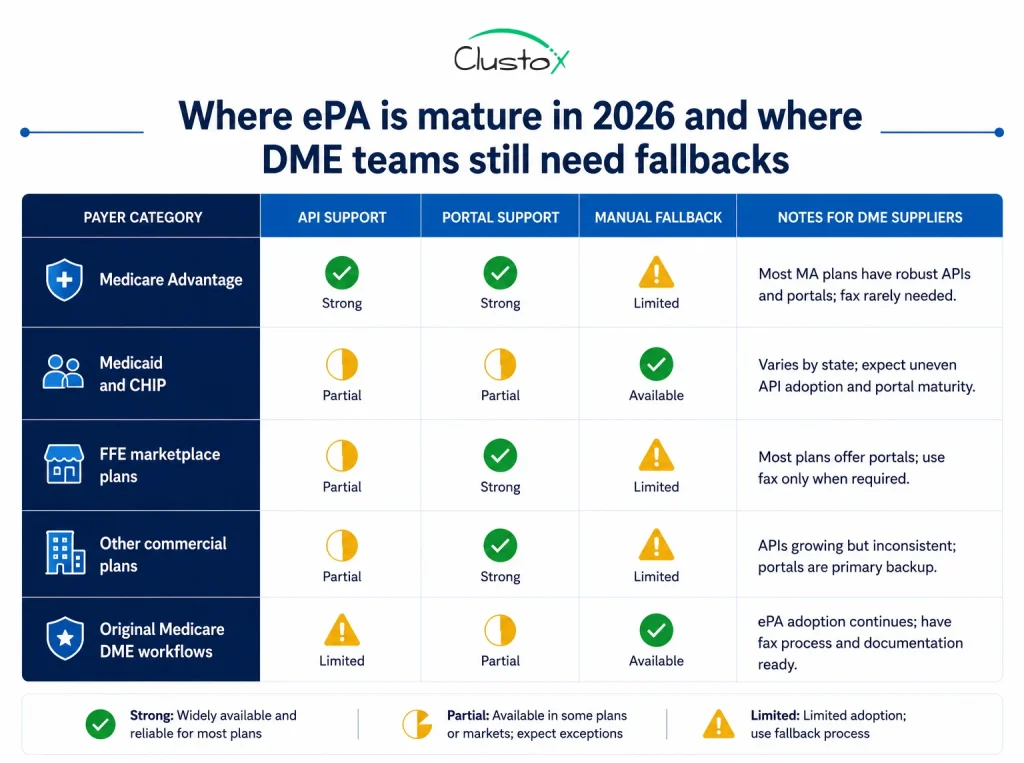
This is where operators need precision. In 2026, payer support for ePA depends less on the buzzword and more on the payer category, the line of business, and whether you are talking about an API, a portal, or a clearinghouse connection.
| Payer category | 2026 reality | Operational takeaway for DME |
|---|---|---|
| Medicare Advantage, Medicaid FFS, Medicaid managed care, CHIP managed care | Subject to CMS-0057-F prior authorization process requirements in 2026. API requirements are primarily due January 1, 2027, depending on payer type. | Expect progress, but not universal end-to-end API behavior in every market today. |
| QHP issuers on the Federally Facilitated Exchanges | Included in the CMS rule scope, but some timing alignment proposals for non-drug items and services were still proposed by CMS on April 10, 2026. | Treat support as plan-specific and confirm the actual submission path before changing workflow. |
| Other commercial plans outside the FFE scope | Not directly covered by CMS-0057-F. | Support varies widely. Many still rely on portal-first or mixed workflows. |
| Original Medicare FFS DME programs | Not the main target of the payer API requirements in CMS-0057-F. | Your team may still work through program-specific documentation and MAC processes instead of a universal ePA API. |
The short version: in 2026, DME suppliers should not assume that ‘electronic prior authorization’ means the same thing across all payers. One payer may support a structured transaction, another may route you through a portal, and a third may still require faxed attachments for edge cases.
That is why payer intake rules and route selection belong at the front of the workflow. Before your team submits anything, the system should know whether the payer accepts an API request, a portal upload, a clearinghouse transaction, or a manual exception path.
ePa vs. Portal-Based vs. Fax-Based Prior Authorization
From an operator’s seat, the real comparison is not electronic versus manual. It is structured electronic exchange versus semi-manual digital work versus paper-first work.
| Model | Strength | Weak point | Best use case |
|---|---|---|---|
| API-based ePA | Best status visibility and better system-to-system consistency | Requires payer support, integration work, and strong exception handling | High-volume payers and repeatable workflows |
| Portal-based prior auth | Faster than fax and often available before full API support | Still heavy on human entry, screenshots, and duplicate tracking | Mid-maturity players or partial digital adoption |
| Fax or email attachment workflow | Works when nothing else does | Poor status visibility, more resubmission risk, weaker audit trail | Low-volume edge cases and payer exceptions |
If your team is still comparing portal usage against fax, the portal usually wins on speed. But if you are choosing a long-term architecture, portal-only is not the endpoint. It keeps the keystrokes and often forces staff to re-enter the same data into the practice management system, the payer site, and the internal work queue.
The better operating model is hybrid. Use structured ePA where the payer supports it, keep portal automation where the payer is not API-ready, and make exceptions visible so leadership can see which payers still consume the most labor.
How Agentic AI Improves ePA Without Removing Human Control?
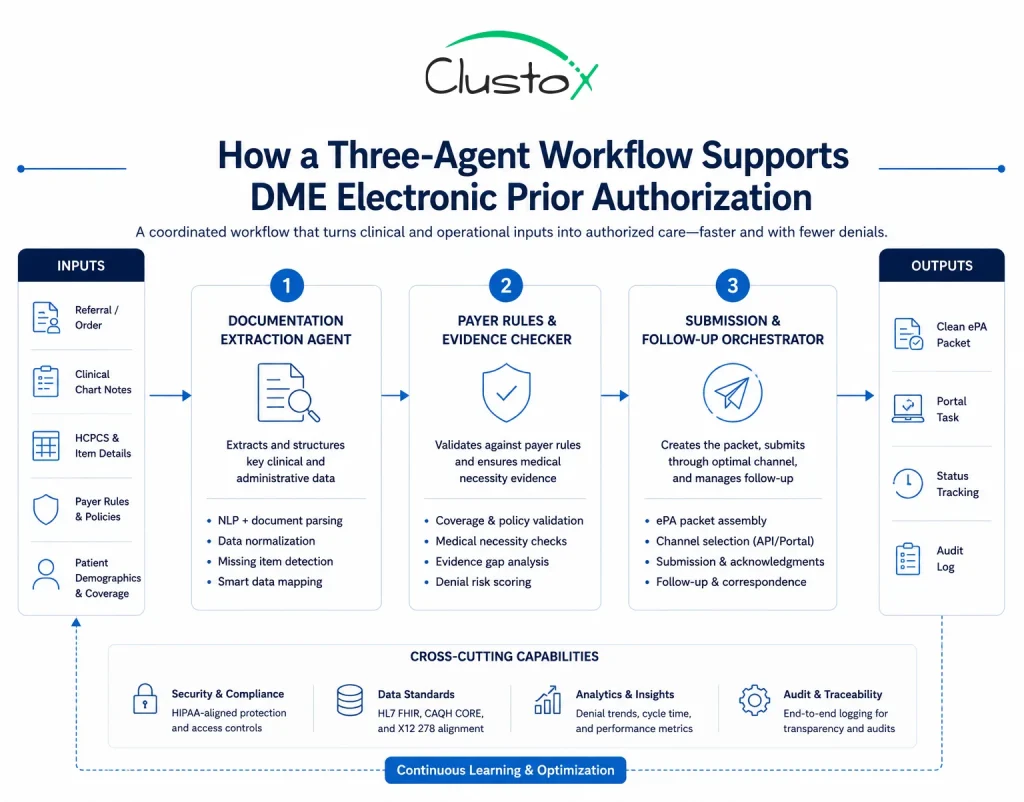
The most useful role for agentic AI in DME prior auth is not blind submission. It is preparation, validation, route selection, and follow-up. The system gathers the order, intake data, diagnosis support, chart notes, and product details, checks what the payer requires, and then prepares the request for staff review or automated handoff.
A practical workflow usually has three layers. First, a documentation agent extracts the fields that matter from referrals, chart notes, and LMN or CMN-related materials.
Second, a rules agent checks payer-specific requirements, missing evidence, and the submission path. Third, a submission agent prepares the payload, portal package, or work queue entry and logs every action for audit purposes.
That approach helps because the heaviest work in DME is often not the final click. It is the manual reading, attachment matching, and chasing of missing evidence before the request is even ready.
Integration patterns with Brightree, NikoHealth, and payer channels
Most DME operators do not need another standalone queue. They need prior auth work to appear inside the operating rhythm they already use.
In practice, that means pulling order and patient context from the PMS, pushing task status back into the PMS, and keeping a linked record of what was sent to the payer.
A clean pattern is the following: PMS creates the work item, integration middleware enriches it with clinical and payer context, the prior authorization workflow determines the route, and status updates flow back to the PMS.
When the payer still requires a portal, the system should at least pre-stage attachments and preserve a structured audit log of who submitted what and when.
This is also where healthcare API integration discipline matters. If the work queue in Brightree or NikoHealth is not the system of record for status, the team ends up reconciling multiple truths. That creates rework and weakens the denial defense later.
1. Compliance, Audit Trail, and Contract Guardrails
Any DME ePA workflow that touches patient data needs the same discipline as the rest of your HIPAA environment. Access controls, minimum necessary data handling, transmission security, retention policy, and vendor contracting still apply whether the request goes through an API, a portal, or a clearinghouse.
Teams building automation around PHI should also understand the role of HIPAA technical safeguards, especially around audit controls, transmission security, access management, and system activity logging.
CMS also raised the floor on denial transparency. Under the 2024 final rule, impacted payers generally must provide prior authorization decisions within 72 hours for expedited requests and seven calendar days for standard requests, and beginning in 2026, they must provide a specific reason for denials for non-drug items and services. That matters because better denial reasons improve resubmission quality.
For Clustox-style implementation work, the control set should include a business associate agreement where needed, role-based access, immutable action logs, exception queues for uncertain cases, and documented escalation when a human reviewer needs to override or add evidence.
2. Implementation Timeline And Cost Reality
The fastest way to stall an ePA project is to treat it like one integration. It is usually four workstreams: payer route mapping, source-system integration, evidence packaging, and operations change management.
| Phase | What happens | What to watch |
|---|---|---|
| Phase 1: workflow mapping | Map payer routes, document sets, denial reasons, and current handoffs. | Do not skip edge cases and low-volume exceptions. |
| Phase 2: system connection | Connect PMS, document sources, and submission channels. | Status write-back matters as much as outbound submission. |
| Phase 3: controlled rollout | Start with a narrow payer set and measure touch time, resubmission rate, and queue aging. | Portal fallback paths need the same audit quality as API paths. |
| Phase 4: scale and governance | Expand to more payers and add playbooks for denials, requests for more information, and escalation. | Governance prevents rule drift and silent failure. |
Cost depends on transaction volume, the number of payer routes you need to support, the condition of your source data, and whether you are integrating with one PMS or several. The better question for leadership is not ‘what does ePA cost?’ It is ‘which work do we stop paying people to do by hand once ePA is in place?’
If you cannot answer that with task-level detail, start with an audit before you buy or build anything.
The Future of DME Prior Authorization
The future of DME prior authorization is steadily moving toward greater interoperability, structured APIs, improved status transparency, AI-assisted workflow orchestration, and more standardized data exchange across healthcare systems.
As payers and providers continue investing in automation, operational analytics, and real-time authorization workflows are expected to become far more common across the industry.
According to the 2025 CAQH Index, the U.S. healthcare industry avoided nearly $258 billion in administrative costs through electronic transactions and improved automation, highlighting how rapidly healthcare operations are evolving toward digital-first workflows.
At the same time, DME providers should expect hybrid operational environments to remain common for years. Many payers still rely on portals, fax-based workflows, manual reviews, and inconsistent documentation requirements, which means complete automation is not yet realistic across every authorization pathway.
Industry research also shows that prior authorization continues to be one of the most time-consuming administrative tasks for providers despite increasing electronic adoption.
The organizations most likely to succeed will not simply be the ones pursuing the most aggressive automation strategies. Success will depend on understanding payer variability, maintaining strong operational governance, preserving audit visibility, integrating workflows effectively, reducing staff burden safely, and using AI strategically instead of recklessly.
The goal is not to remove human oversight entirely, but to build smarter operational systems that improve efficiency while maintaining compliance, transparency, and operational control.
Frequently Asked Questions FAQ
2. How Does ePA Work for DME?
A DME team collects orders and clinical evidence, checks the payer route, submits through the supported channel, and then tracks requests for more information, approval, or denial in a structured workflow.
3. Which Payers Support ePA for DME?
Support varies by payer category and line of business. In 2026, CMS process requirements apply to Medicare Advantage, Medicaid, and CHIP programs and QHP issuers on the Federally Facilitated Exchanges, but the API rollout is still maturing, and other commercial plans vary widely.
4. Is Electronic Prior Authorization Required?
Not across every DME workflow. Some payer categories are under CMS requirements, but suppliers still face mixed submission paths in 2026.
5. Can AI Submit ePAs Automatically?
It can prepare, validate, package, and route requests, and in some workflows, it can trigger structured submission. High-risk cases still need human review and explicit escalation rules.
6. What Standards Govern ePA?
For medical-benefit workflows, think X12 278, HL7 FHIR Da Vinci PAS, and CAQH CORE operating rules. For pharmacy-benefit ePA, NCPDP standards matter.
7. How Long Does Epa Take Compared With Fax?
ePA usually reduces re-entry and improves status visibility, but actual turnaround depends on payer response time, documentation quality, and whether the route is truly structured or just portal-based.
Conclusion
Electronic prior authorization is worth pursuing in DME because it turns an opaque, staff-heavy process into something you can measure and improve. But in 2026, the winning approach is not to assume every payer is API-ready. It is to build a route-aware workflow that handles APIs, portals, and exceptions without losing audit quality.
If your team wants to know where ePA can reduce labor first, working with a reliable software development service partner can help identify which payer routes, document types, and operational queues are ready for automation today and which still need workflow cleanup before scaling.
Audit Your DME Prior Authorization Workflow
Clustox has helped healthcare teams cut through prior authorization complexity with AI-driven automation and interoperability solutions built for real DME workflows.