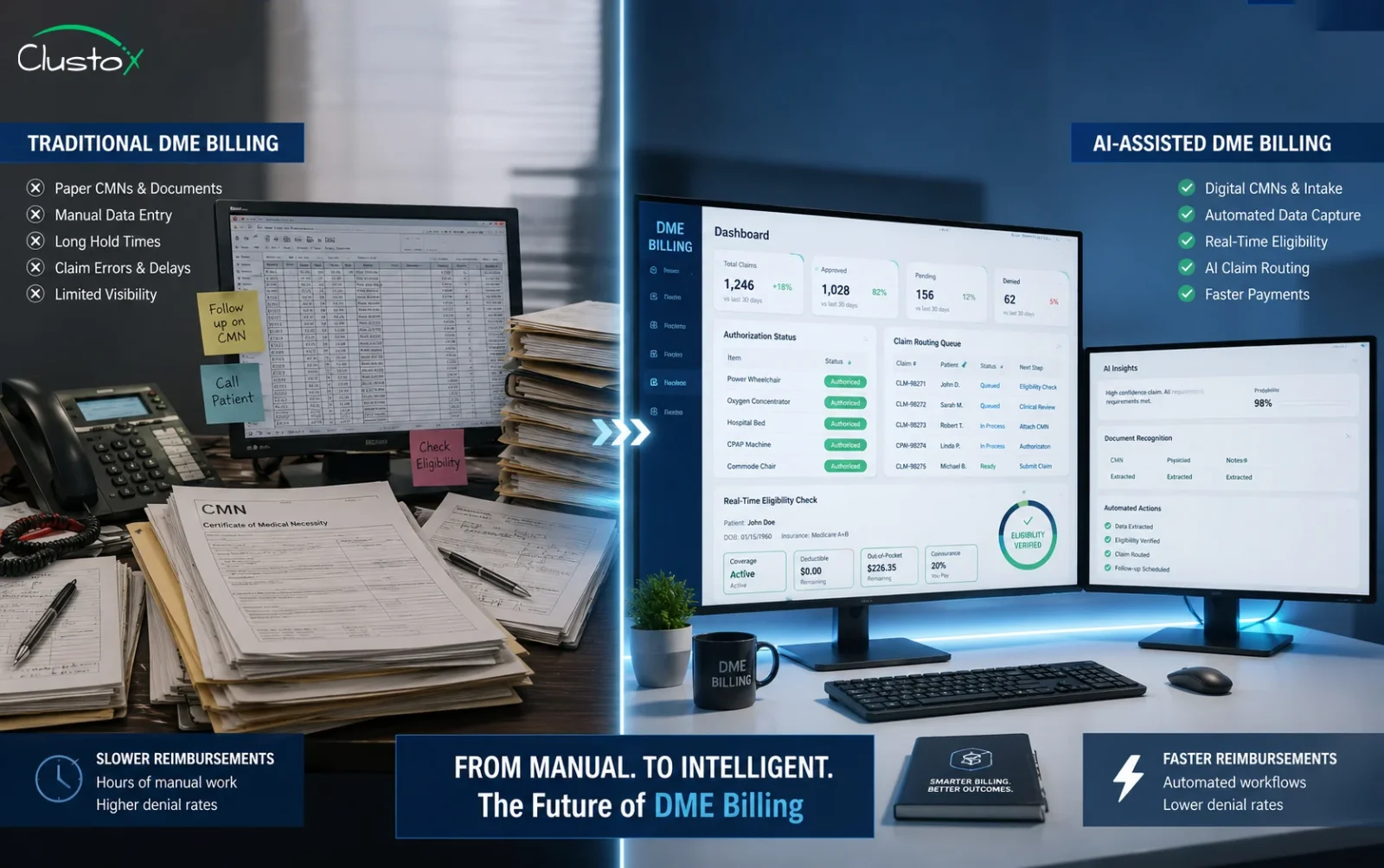
AI-assisted medical billing software for DME automates the tasks that drain your billing team the most: prior authorization, eligibility verification, claim scrubbing, and denial follow-up. The result is faster reimbursements, fewer denials, and less manual work per claim.
If you run billing for a DME company, you already know what this job costs. Claims touch multiple payers, each with their own documentation requirements. Prior auth can take anywhere from three to ten business days. Denials come back with vague codes and no clear path to fix them. Your team spends hours on tasks that should take minutes.
Medical billing software has been around for years. What is different now is what AI can actually do inside these platforms. It is not a marketing layer on top of old tools. In the right implementations, it changes the throughput of your revenue cycle in ways that were not possible before.
AI is changing how DME providers manage billing workflows, documentation, and reimbursements through AI-powered healthcare workflow automation.
This guide covers what AI-assisted DME billing software does, which workflows it changes the most, what to look for when you evaluate platforms, and what the honest limitations are. You can read it start to finish or jump to the section most relevant to where you are right now.
What Does Medical Billing Software for DME Actually Do?
DME billing is more complex than standard medical billing. You are dealing with HCPCS codes, certificate of medical necessity documentation, Medicare and Medicaid requirements, private payer contracts, and a prior authorization process that varies by payer and equipment type. Standard medical billing software was not built with these workflows in mind.
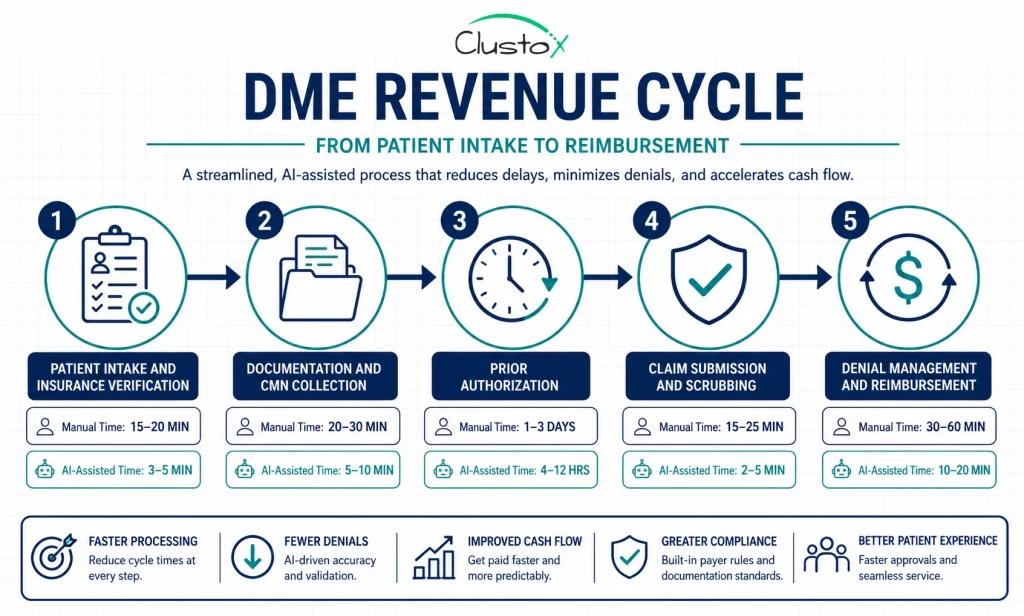
Table of Contents
DME-specific billing software handles:
- Patient intake and insurance eligibility checks
- CMN and documentation tracking
- Prior authorization submission and follow-up
- HCPCS coding and claim scrubbing
- Electronic claim submission to Medicare, Medicaid, and commercial payers
- Denial management and appeal tracking
- Reimbursement posting and accounts receivable reporting
Platforms like Brightree, NikoHealth, TIMS, and Universal Software Solutions have covered most of these functions for years. What AI adds is the ability to automate the decision points that used to require a billing specialist to review manually.
Which DME Billing Tasks Does AI Automate Today?
The honest answer is: a lot, but not everything. Here is what AI is doing reliably in production DME billing environments today.
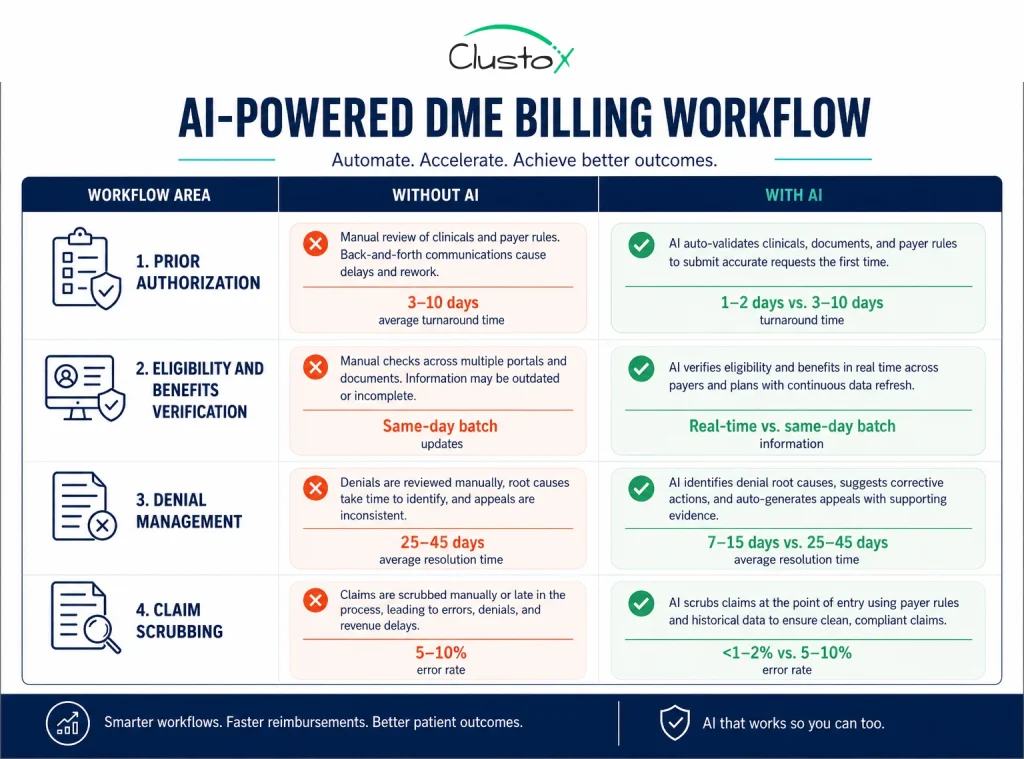
Prior authorization
Prior authorization is where most DME companies lose the most time. Manually, it involves pulling the right payer form, pulling documentation from the EHR or physician’s office, filling out the request, submitting it, and then following up. That cycle takes three to ten business days on average with manual workflows.
AI agents can pull the payer’s current criteria, check the patient’s documentation against those criteria, flag gaps before submission, and submit the request automatically. Follow-up reminders and status checks can also be automated. The realistic target with a well-built AI workflow is one to two business days.
Eligibility and benefits verification
Real-time eligibility verification is not new, but AI adds a layer on top. Instead of just returning a benefits summary, newer platforms can parse the response, identify secondary payers, flag coverage gaps for specific equipment categories, and surface the information your team needs to bill correctly the first time.
Denial management
Denial management is where AI has the most room to improve outcomes. Most DME billing teams handle denials reactively. They see a denial code, look up the reason, decide whether to appeal, write the appeal, and re-submit. That is a slow loop. AI can classify denial reasons automatically, prioritize by dollar amount and appeal success probability, and draft the appeal using the correct supporting documentation. Your team reviews and approves instead of starting from scratch each time.
Claim scrubbing
AI-driven claim scrubbing can catch coding errors, missing modifiers, and documentation mismatches before a claim goes out the door. The more valuable feature is predictive: some platforms can flag claims that are likely to be denied based on historical payer patterns, even if there is no hard rule violation.
How Does AI-Assisted Prior Authorization Work in DME Billing?
Prior auth is the single biggest time drain in most DME billing departments. Understanding how AI handles it is worth a closer look.
The traditional process relies on a billing specialist who knows each payer’s requirements, has the right forms, can track submission status, and manages follow-up calls. That knowledge lives in people, not systems. When those people are out or when volume spikes, the process breaks.
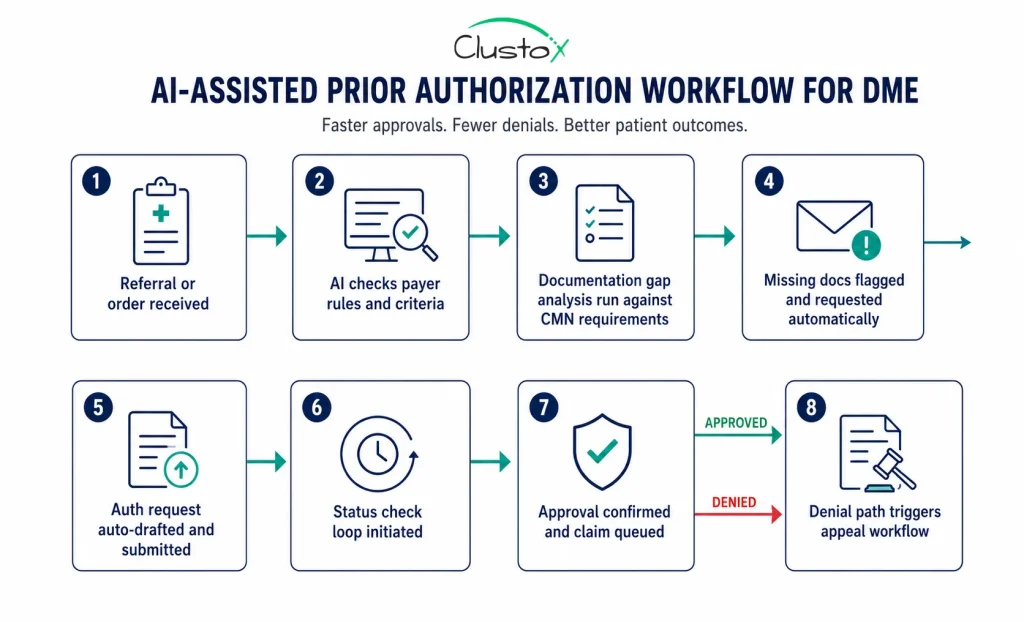
An AI-assisted prior auth workflow works differently:
- The order or referral comes in and the system identifies the payer and equipment type.
- The AI checks the payer’s current prior auth criteria (some platforms maintain live payer rule libraries).
- It runs a documentation gap check against what is already in the patient file.
- Missing documentation is flagged and, in some implementations, automatically requested from the referring physician’s office.
- The auth request is drafted and submitted through the payer’s portal or clearinghouse.
- Status checks are automated on a defined schedule. No one has to remember to follow up.
- An approval triggers automatic claim queuing. A denial triggers the appeals workflow.
The key difference is that the system holds the process state, not a person. Volume spikes do not create backlogs the same way. New staff do not need to learn payer-by-payer rules from scratch. And when a payer changes their criteria, the update propagates across all submissions.
What Features Should You Look for in DME Billing Software?
Not every platform that calls itself AI-powered has the same depth.
Here is what actually matters when you are evaluating medical billing software for a DME operation.
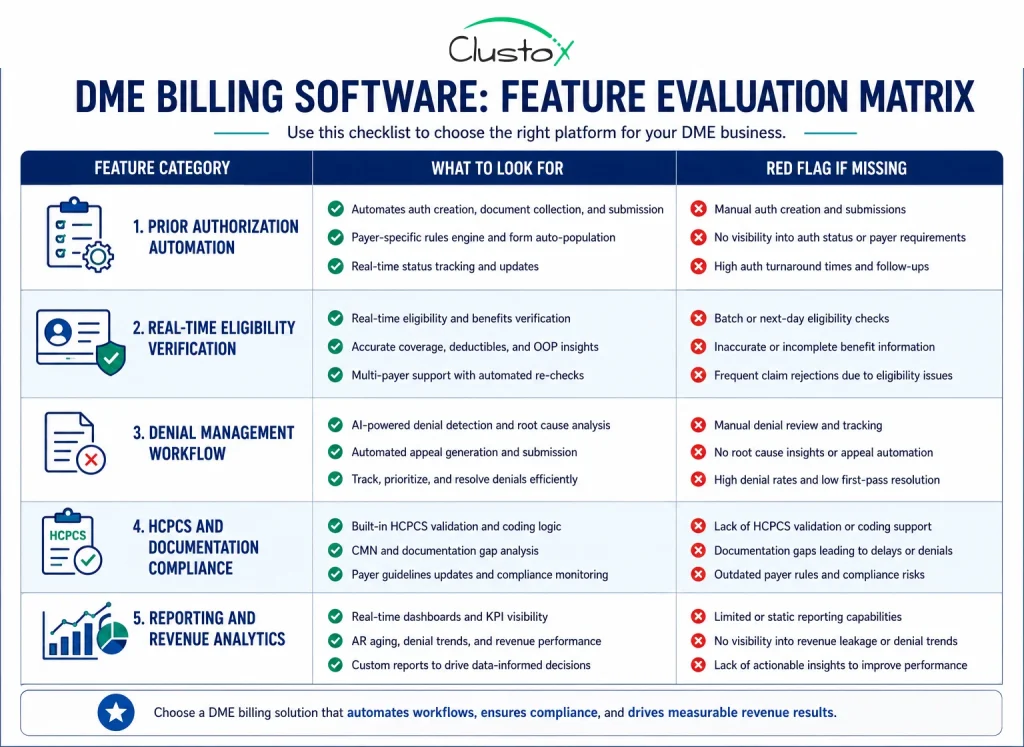
Payer rule library depth and update frequency
AI-assisted prior auth is only as good as the payer rules it is working from. Ask vendors specifically how they maintain their payer rule library, how often it is updated, and whether rules are validated against live payer policies or manually curated. A stale rule library creates the same errors as manual work, just faster.
Integration with your DME management platform
If you are on Brightree, NikoHealth, or another platform, the billing software needs a clean data connection. Manual exports and imports between systems create errors and negate most of the automation value. Confirm exactly which data fields pass between systems and in which direction.
Denial analytics with action workflows
Reporting on denial rates is baseline. What you actually need is a system that classifies denials, tracks them back to root causes, and gives your team a clear next step. If the denial management feature just shows you a report without driving action, it is not solving the problem.
Documentation compliance checks
CMS documentation requirements for DME are detailed and frequently updated. The software should flag documentation issues before a claim is submitted, not after it is denied. This includes checking for LMN completeness, correct HCPCS modifiers, and CMN signature requirements.
Configurable workflows for your billing model
Your billing operation is not the same as every other DME company’s. If the platform only supports one workflow model, you will spend a lot of time working around it. Look for configurable automation rules that map to your actual processes.
How Do Leading DME Billing Platforms Compare?
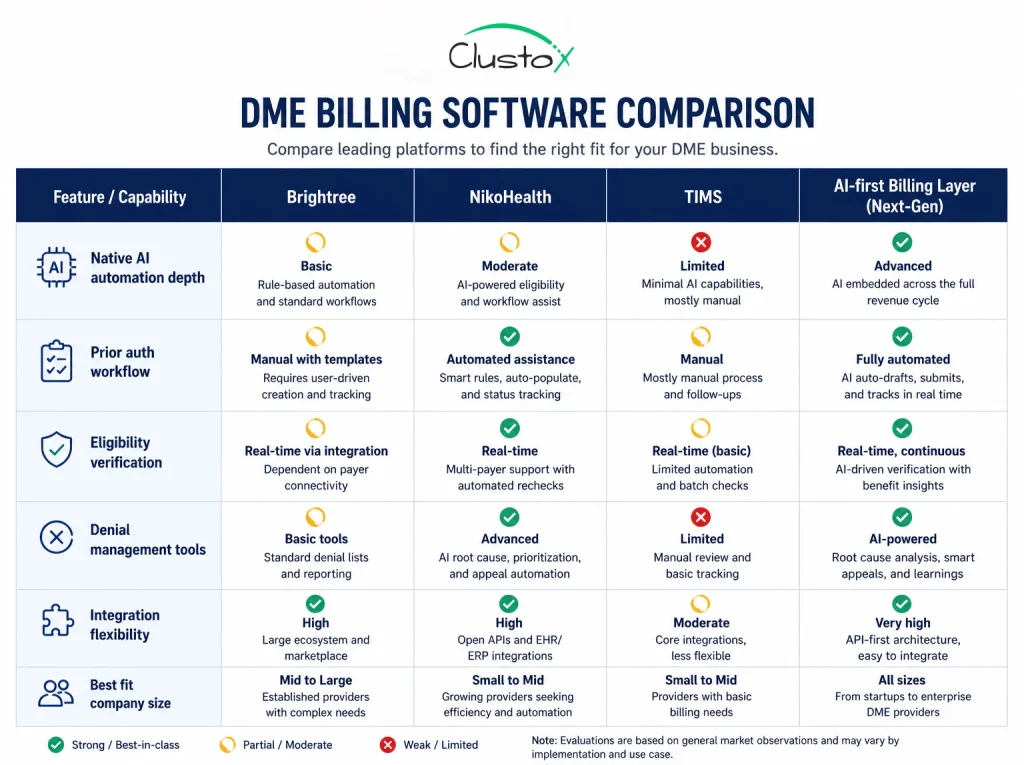
This section gives you a working comparison. It is not exhaustive, and platform capabilities change. Treat this as a starting framework, not a final verdict. Always verify current features directly with vendors.
| Platform / Approach | What it does well in DME billing |
|---|---|
| Brightree | Deep DME workflow coverage, strong resupply automation, widely adopted by mid-to-large providers. AI features expanding, but native depth varies by module. |
| NikoHealth | Modern interface, designed for DME from the ground up, growing AI feature set including eligibility and documentation workflows. Strong for providers scaling off legacy systems. |
| TIMS | Long-standing DME billing tool with solid Medicare and Medicaid claim handling. More traditional in architecture. Best evaluated for fit if your team is already on it. |
| AI-layer / custom workflow | For operations that have already chosen a core DME platform but want deeper AI automation on top, a purpose-built AI billing layer can handle prior auth, denial management, and documentation workflows independently of the core platform's native AI maturity. |
The right choice depends on your current platform, team size, payer mix, and how much process change your operation can absorb in a given period. A platform that is technically superior but requires six months of onboarding may not outperform a lighter-touch integration that goes live in weeks.
What Are the Real Benefits of AI in DME Medical Billing?
Here is what actually changes when AI is working well inside a DME billing operation.
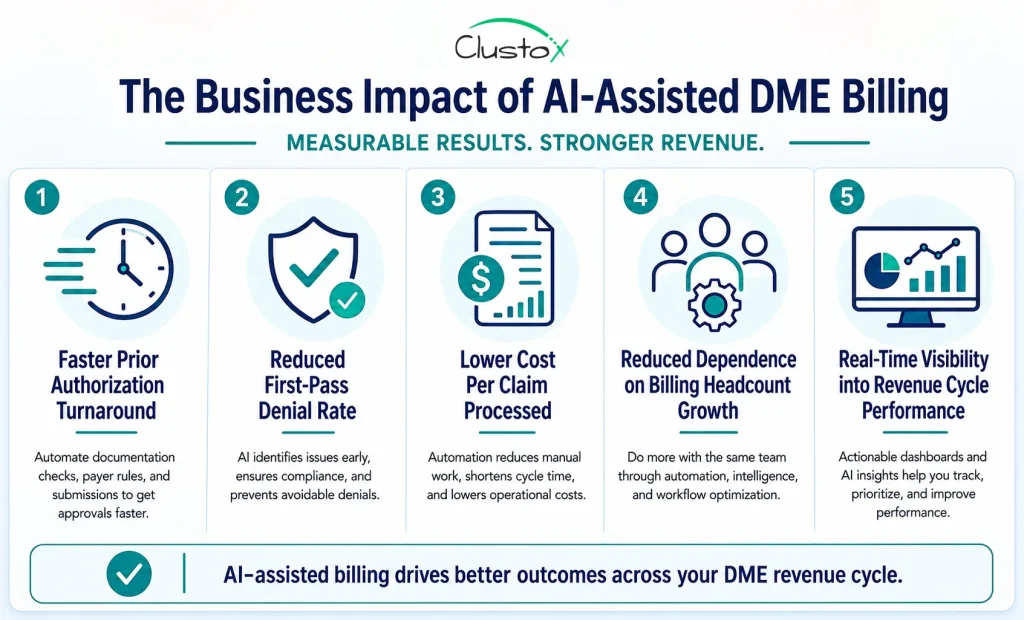
Fewer denials on the first submission
When AI checks documentation completeness and payer rule compliance before a claim goes out, the first-pass denial rate drops. The financial impact compounds quickly because denied claims cost time to rework and often result in delayed or lost reimbursement.
Faster prior authorization
Moving from three to ten business days down to one to two days on prior auth is not just a speed improvement. It means your DME reaches patients sooner, your team spends less time on status calls, and your cash flow cycle shortens.
Lower cost per claim
When your billing team spends less time on manual verification, documentation collection, and denial rework, the cost to process each claim goes down. That is more meaningful for scaling operations than it might appear: cost per claim is one of the clearest indicators of billing department efficiency.
Staff capacity shifts toward higher-value work
The goal is not to eliminate billing staff. The goal is to shift what they spend their time on. When AI handles routine verification and follow-up, your experienced billers can focus on complex payer escalations, contract issues, and accounts that actually require human judgment.
Better visibility into where claims are
AI-driven dashboards give your billing director and CFO a real-time view of where claims sit in the cycle: what is pending authorization, what is in scrubbing, what is in denial, and what is awaiting resubmission. That visibility is hard to get from manual tracking.
What Are the Limitations of AI in DME Billing?
This section exists because most vendor material will not tell you what does not work. Here is an honest assessment.
AI is only as good as your data
If your patient records are incomplete, your EHR integration is unreliable, or your documentation workflows are inconsistent, AI automation will surface those problems rather than solve them. You are not buying a fix for data quality issues.
Payer behavior is unpredictable
Even well-maintained payer rule libraries have gaps. Payers change their requirements, sometimes without clear advance notice. An AI that was processing a certain payer’s auth correctly last month may fail next month if the rules changed and the library has not updated. Human review remains important for edge cases.
Implementation takes real effort
Platforms that promise fast go-live times often mean fast to basic functionality. Deep AI automation in prior auth and denial management typically requires process mapping, configuration, staff training, and a period of parallel running before you can trust the automation fully.
Compliance risk does not disappear
AI can reduce documentation errors, but it does not eliminate compliance risk. Billing staff still need to understand CMS requirements. Audit risk is a function of your documentation, your coding accuracy, and your payer relationships. AI improves the inputs; it does not remove the need for compliance oversight.
ROI timelines vary
Vendors will show you best-case ROI scenarios. The actual timeline depends on your starting denial rate, your current cost per claim, how smoothly the implementation goes, and how quickly your team adopts the new workflows. Set realistic expectations and measure from a clear baseline.
How Should You Evaluate and Implement New Billing Software?
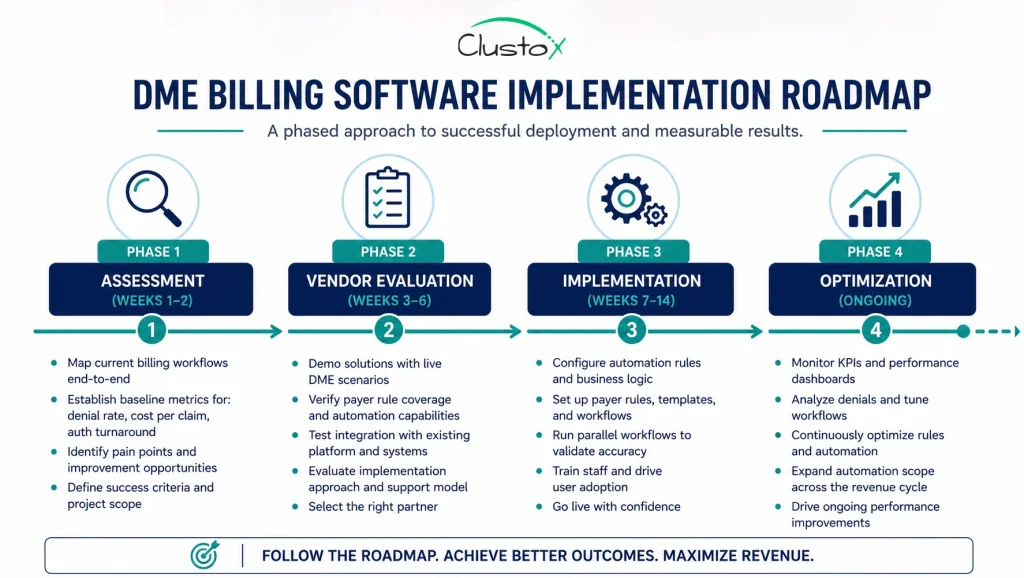
Choosing the right platform matters less than implementing it correctly.
Here is a practical framework.
Start with a baseline measurement
Before you evaluate any platform, document your current metrics: first-pass denial rate, average prior auth turnaround time, cost per claim, and days in accounts receivable. Without this baseline, you cannot measure whether anything improved.
Test vendors with real DME scenarios
Generic demos are not useful. Bring a set of realistic scenarios: a specific payer’s prior auth requirements, a denial code you commonly receive, and a documentation gap situation. Ask the vendor to walk through how their platform handles each one. The quality of that walkthrough tells you more than any feature list.
Ask about payer rule maintenance
This is the question most buyers forget. Ask the vendor: How do you maintain your payer rule library? How quickly do you update rules when CMS or a major payer changes requirements? Who is responsible for that process? The answer separates platforms that work in year one from those that degrade over time.
Plan for an integration validation phase
Before you go live on automation, run a period where AI-generated outputs are reviewed by your billing team before submission. This validation period lets you catch configuration errors and edge cases before they affect claim volume. It typically takes four to eight weeks for a mature implementation.
Define the metrics you will track monthly
Commit to tracking denial rate, prior auth turnaround, and cost per claim on a monthly basis from day one. If those numbers are not improving after 90 days, something in the configuration or the workflow adoption needs to change.
DME Billing Software Buyer’s Checklist
Use this before you make a final decision on any platform.
Vendor evaluation checklist
Integration and data
- Confirmed direct integration with your current DME management platform (Brightree, NikoHealth, TIMS, etc.)
- Defined data fields that pass between systems, validated with a live test
- Clear data ownership and HIPAA compliance documentation
Prior authorization:
- Live payer rule library covering your top 10 payers by claim volume
- Demonstrated update process for payer rule changes
- End-to-end prior auth automation tested with a real scenario from your payer mix
Denial management:
- Denial classification with root cause tagging, not just code display
- Appeal workflow with auto-drafted appeal letters reviewed and confirmed
- Denial trend reporting by payer, code, and time period
Compliance and documentation:
- Pre-submission documentation compliance check against CMS requirements
- HCPCS modifier validation built in
- CMN and LMN completeness checks confirmed
Implementation and support:
- Named implementation contact with DME billing experience
- Defined go-live timeline with parallel-run phase included
- Escalation path for payer rule gaps discovered post-launch
Frequently Asked Questions
How is AI used in DME billing software?
AI is used primarily in three areas: prior authorization (checking payer rules, identifying documentation gaps, and automating submission), denial management (classifying denial reasons and drafting appeals), and claim scrubbing (identifying coding errors and documentation issues before submission). The depth of AI automation varies significantly between platforms.
Does AI billing software reduce prior auth turnaround time?
Yes, in well-implemented cases. Manual prior auth typically takes three to ten business days. AI-assisted workflows can bring this down to one to two days by automating payer rule checks, documentation gathering, and submission. The actual improvement depends on payer response times, which AI cannot control.
What is the difference between DME billing software and general medical billing software?
DME billing involves HCPCS codes, CMN documentation, Medicare and Medicaid supplier standards, and prior authorization processes that are specific to equipment suppliers. General medical billing software handles CPT codes and physician office billing workflows. The two overlap in some areas but DME providers routinely find that general platforms miss critical DME-specific compliance checks.
Is Brightree considered AI-powered billing software?
Brightree is a full DME management platform with billing capabilities. It has been expanding AI features, but the depth of native AI automation varies by module and continues to evolve. Providers evaluating Brightree for AI-assisted billing should review current features directly with the vendor and consider whether a supplemental AI layer adds value for their specific workflows.
How long does it take to implement DME billing software?
Basic implementation can go live in four to eight weeks. Full AI automation in prior auth and denial management typically takes twelve to sixteen weeks when you include configuration, parallel-run validation, and staff training. Compressed timelines tend to produce configuration gaps that show up as claim errors post-launch.
What metrics should I track after implementing AI billing software?
Track first-pass denial rate, prior authorization turnaround time, cost per claim, and days in accounts receivable. Set a baseline before you go live so you have a real comparison. Monthly tracking for the first six months gives you enough data to identify whether the automation is working or needs adjustment.
Can AI billing software integrate with my existing DME management platform?
Most purpose-built DME billing platforms offer integration with major systems like Brightree and NikoHealth. The quality of the integration, meaning which data fields pass, how reliably, and in which direction, varies. Before committing to a vendor, validate the integration with a live test using your actual platform and data.
Will AI billing software reduce the number of billing staff I need?
Not necessarily, and that framing can lead to the wrong implementation decisions. AI removes routine manual tasks from your billing team's workload. The realistic outcome is that the same team handles more claims with fewer errors, or that you can scale claim volume without proportional headcount growth. Billing specialists still handle complex denials, payer escalations, and compliance oversight.
The Bottom Line on AI and DME Billing Software
Medical billing software for DME has been available for years. What is different now is the quality and reliability of the AI embedded in these platforms. For prior authorization, denial management, and claim scrubbing, AI automation has matured to the point where it is worth evaluating seriously, not as a future investment but as an operational choice you can make this year.
The providers getting the most value from it are not the ones who bought the most expensive platform. They are the ones who mapped their current billing workflows before they bought anything, set a measurable baseline, and implemented the automation in stages with a proper validation phase.
If your prior auth backlog is holding up equipment delivery, if your denial rate is running above industry norms, or if your cost per claim keeps rising as you add volume, these are the indicators that AI-assisted billing is worth a serious look.
Want to see what AI-assisted billing looks like in your DME operation?
Clustox helps DME providers modernize billing operations with AI-powered automation that reduces denials, speeds up payments, and scales with growing patient demand.
This article is intended for DME providers, operations leaders, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, accreditation standards) are accurate as of the review date. Regulations change frequently and providers should consult primary sources or qualified counsel for current requirements.