Picture this: your billing team submits 400 claims this month. By the time remittance comes back, 72 of them are denied. That is not a rounding error; that is $25,200 in revenue your operation earned, delivered, and documented, now sitting in a work queue waiting for someone to fight for it.
Most DME operators accept this as the cost of doing business. They hire more billing staff, build bigger denial queues, and absorb the write-offs that the team never gets to.
What they rarely do is ask the harder question: why is the denial rate 18% in the first place, and how much of it is the software’s fault?
The answer is uncomfortable. A significant portion of DME claim denials, conservatively 60–70%, by root cause trace back to workflow failures that the right claims processing software would have caught before the claim ever left the building. Wrong HCPCS modifier. Eligibility not re-checked. Prior auth on file for the wrong date range. Documentation that nobody actioned. These are not complex clinical judgment calls. They are process failures, and process failures are fixable.
This guide is for the DME operator who is tired of treating a 15–18% denial rate as normal. It explains exactly why DME claims get denied at nearly double the healthcare industry average, which software features prevent the most common denial categories, and what to look for when evaluating platforms or deciding whether to add an AI layer on top of the system you already have.
What this Guide Covers:
- Why DME claim denial rates are nearly double the healthcare industry average
- The 7 root causes behind the 18% denial rate, which are fixable at the software level
- Core feature requirements for DME claims processing software in 2026
- How leading platforms (Brightree, NikoHealth, TIMS) handle claims differently
- What AI-layer tools add on top of core billing software
- A buyer’s checklist for evaluating vendors
- Real denial reduction benchmarks from DME operators
Why DME claim denial rates run higher than the rest of healthcare
The healthcare billing industry’s average first-pass denial rate sits around 9–10%, according to HFMA’s 2023 Revenue Cycle Benchmarking Report. DME suppliers routinely see 15–18%, and for smaller operators without dedicated billing staff, denial rates above 20% are not uncommon.
DME billing carries structural complexity that most other healthcare billing doesn’t:
Table of Contents
- Documentation burden: Every order requires a detailed written order (DWO), proof of delivery (POD), and in many cases a Letter of Medical Necessity (LMN). Missing or non-compliant documentation is the single largest denial driver.
- HCPCS code specificity: DME reimbursement is tied to HCPCS Level II codes, many of which have modifier requirements (KX, GA, GY, GZ) that must be applied correctly or the claim rejects.
- Payer rule proliferation: Medicare Part B, Medicare Advantage, Medicaid, and commercial payers each maintain separate coverage determination policies for the same equipment. A power wheelchair (K0856) covered under Medicare may be denied under a specific Medicare Advantage plan for the same patient.
- Prior authorization requirements: CMS expanded the prior authorization program for certain DME categories under 21st Century Cures Act provisions. Missing or expired PAs are an automatic denial.
- Rental vs. purchase rules: Inexpensive or routinely purchased items have different billing rules than capped rental items (oxygen equipment, CPAP, wheelchairs). Billing a capped rental item as a purchase, or miscounting rental months, triggers claim rejection.
Denial rate snapshot: DME vs. healthcare average
9–10% Healthcare industry average first-pass denial rate (HFMA, 2023)
15–18% DME supplier average first-pass denial rate (HFMA DME cohort)
20%+ Denial rates common for DMEs without dedicated claims processing staff
$118 Average cost per denied claim when accounting for rework, appeals, and write-offs (HFMA)
$2.5B+ Estimated annual DME revenue at risk from preventable denials (AAHomecare, 2023)
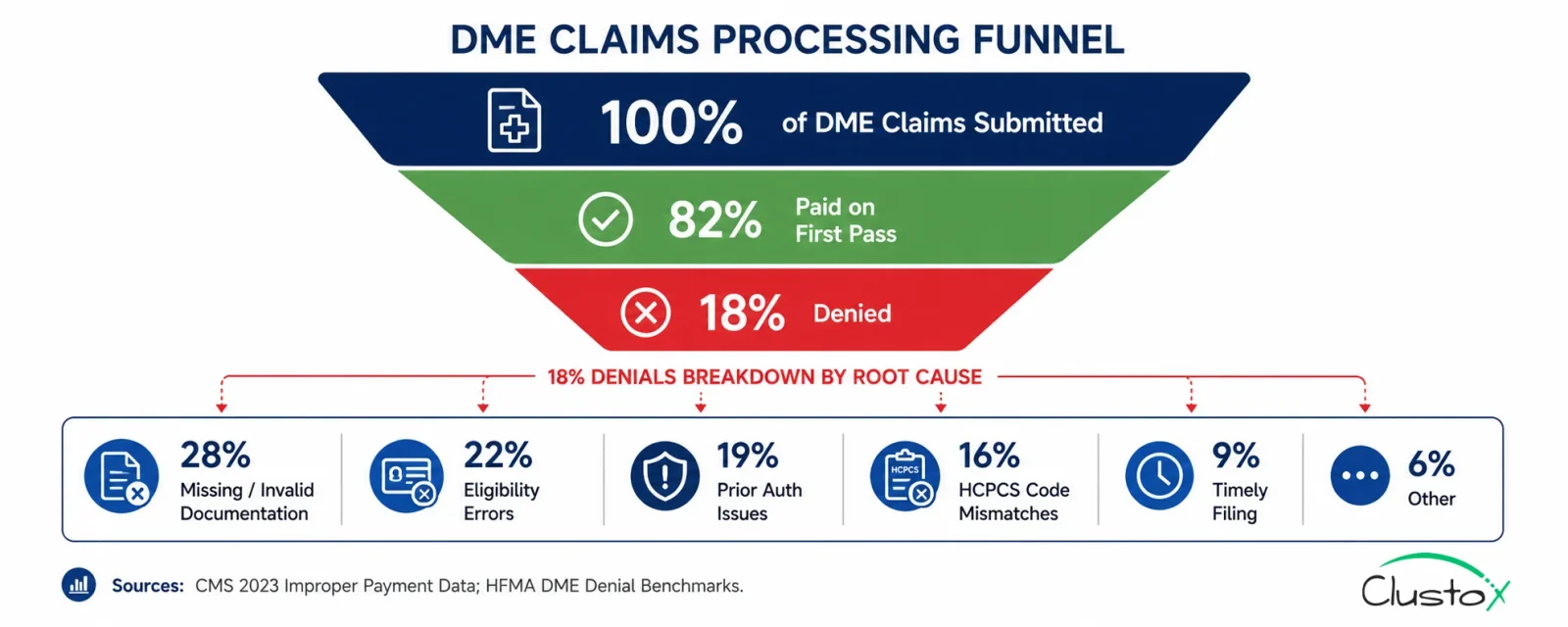
The 7 root causes behind the 18% DME denial rate
| Denial Root Cause | Share of DME Denials | Fixable at Software Level? |
|---|---|---|
| Missing or non-compliant documentation (DWO, POD, LMN) | ~28% | Partially software can flag gaps; documentation still requires clinical input |
| Eligibility and coverage errors | ~22% | Yes automated eligibility verification eliminates most of these |
| Prior authorization missing or expired | ~19% | Yes PA tracking and auto-queue prevents the majority |
| HCPCS code mismatch or wrong modifier | ~16% | Yes HCPCS intelligence layer catches coding errors pre-submission |
| Timely filing violations | ~9% | Yes automated claim submission queues eliminate filing delays |
| Duplicate claim submission | ~4% | Yes deduplication logic in claims software prevents these |
| Other (wrong NPI, rendering provider errors, etc.) | ~2% | Yes data validation rules catch these at entry |
Source: HFMA DME denial benchmark cohort; CMS 2023 Medicare Fee-for-Service Improper Payment Data. Note: shares are approximate and vary by payer mix and provider type.
How claims processing software works in a DME operation
Claims processing software for DME handles the full revenue cycle loop from order creation to remittance posting.
The core workflow runs in seven steps:
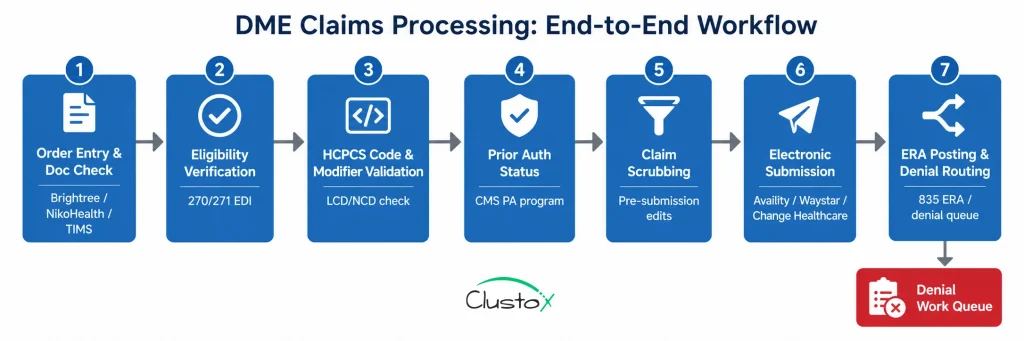
- Order entry and documentation check: The order is created in Brightree, NikoHealth, or TIMS. The system checks for required documentation fields (DWO, LMN, POD status, referring physician NPI).
- Eligibility verification: The system submits a 270/271 EDI transaction to confirm active coverage, HCPCS benefit eligibility, and prior auth requirements for the specific payer and plan.
- HCPCS code assignment and modifier validation: Codes are assigned (manually or via AI-assisted suggestion) and checked against the payer’s local coverage determination (LCD) and national coverage determination (NCD) policies.
- Prior authorization status check: The system confirms whether a PA is required, whether one is on file, and whether it covers the order date and HCPCS code.
- Claim scrubbing: Pre-submission edits catch formatting errors, missing fields, invalid modifiers, and timely filing risk. Claims that fail scrubbing route to a work queue for correction.
- Electronic claim submission: Clean claims submit via clearinghouse (Availity, Waystar, Change Healthcare) to the appropriate payer. Acknowledgment (277CA) is captured and logged.
- ERA posting and denial management: Electronic Remittance Advice (835 ERA) is auto-posted. Denied claims route to a denial work queue with denial reason codes, payer notes, and recommended next actions.
How do Brightree, NikoHealth, and TIMS handle DME Claims Differently?
The three dominant DME billing platforms each take a different architectural approach to claims management. Understanding the differences matters when you’re evaluating whether to add an AI layer on top of your existing system or switch platforms.
| Feature | Brightree | NikoHealth | TIMS Medical |
|---|---|---|---|
| Market positioning | Enterprise and mid-market DME/HME | Mid-market, cloud-native | Small-to-mid, legacy-friendly |
| Claims scrubbing | Built-in, configurable rule sets | Built-in with payer-specific profiles | Built-in; less frequently updated |
| ERA auto-posting | Yes, via integrated clearinghouse | Yes | Yes, with manual reconciliation fallback |
| Prior auth tracking | Module included | Module included | Basic tracking; manual-heavy |
| HCPCS code intelligence | Rule-based; limited AI assist | Rule-based | Rule-based |
| AI/automation layer | Supported via API (third-party) | Supported via API (third-party) | Limited API access |
| Denial management workflow | Configurable queues; strong reporting | Configurable queues | Basic denial queue |
| Clearinghouse integration | Waystar (native), Availity, Change | Waystar, Availity | Waystar, Change Healthcare |
Note: Feature parity changes with software releases. Verify current capabilities directly with each vendor. CMS maintains a list of approved DME billing software resources via the Medicare Learning Network (MLN).
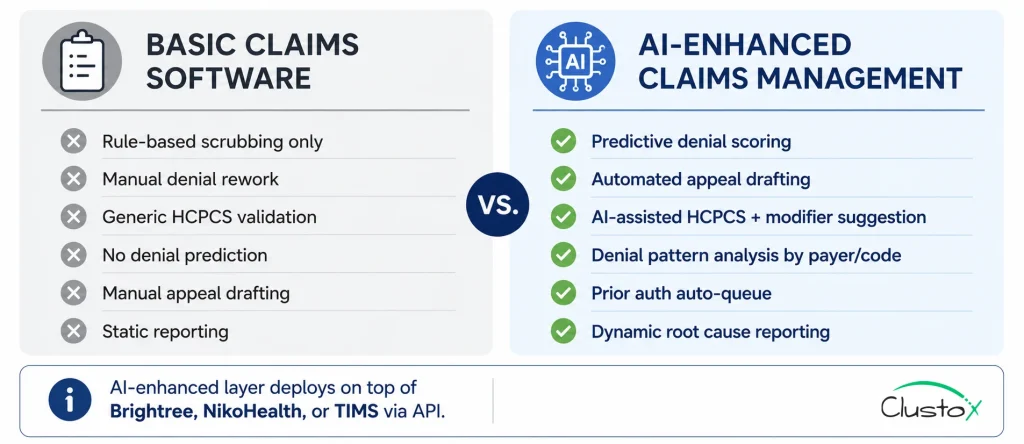
What An AI Layer Adds On Top Of Core Claims Processing Software
Brightree, NikoHealth, and TIMS handle the structural claims workflow well. What they don’t do is reduce the human decision-making burden on the exception queue or learn from denial patterns to prevent recurrence. That’s where an Agentic AI layer built on top of the core platform via API adds material value.
1. Denial prediction scoring
An LLM-based agent can score each claim before submission based on historical denial patterns for that payer, HCPCS code, and documentation set. Claims above a denial risk threshold route to a pre-submission review queue rather than submitting and failing. Operators using denial prediction scoring report 12–18% reductions in first-pass denial rates within 90 days of deployment.
HCPCS code intelligence
AI-assisted HCPCS coding reviews the order, clinical notes, and referring provider documentation to suggest the correct HCPCS code and required modifiers and flags cases where KX modifier attestation is required but the clinical documentation doesn’t clearly support it. This reduces the volume of GA and GY modifier errors that trigger medical necessity denials. Reference: CMS HCPCS code set lookup and LCD policies.
Automated appeals drafting
When a claim is denied and the denial is appealable, an AI agent can draft the appeal letter, pull the relevant LCD/NCD policy text, reference the specific documentation on file, and route it to the billing manager for review and submission. Appeal drafting time drops from 45–60 minutes per appeal to under 10 minutes for standard denial types.
Denial pattern analysis and root cause reporting
A RAG-based analytics agent can identify recurring denial patterns across payer, code, and referring provider and surface the operational fix. For example: if 40% of denials from a specific Medicare Advantage plan involve modifier KX on CPAP equipment, the agent can flag that the LMN template used for that equipment type isn’t capturing the required qualifying language.
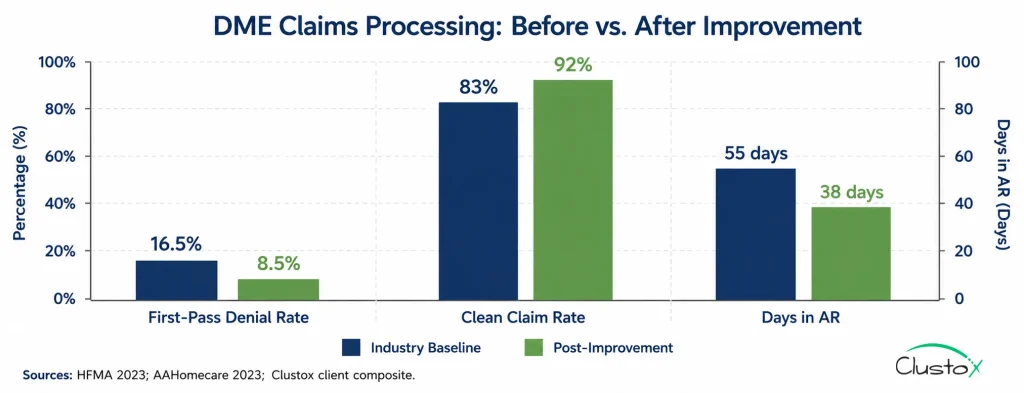
Real numbers: what DME operators see after improving claims processing
The benchmarks below reflect operator-reported outcomes following implementation of structured claims processing improvements either platform upgrades, AI layer additions, or both.
Individual results vary by payer mix, starting denial rate, and implementation quality.
| Metric | Baseline (Industry Avg) | Post-Improvement | Notes |
|---|---|---|---|
| First-pass claim denial rate | 15–18% | 7–10% | Achievable within 6–12 months; requires documentation and eligibility fixes alongside software |
| Cost to collect per claim | $8–14 | $5–9 | Reduction driven by fewer rework cycles and appeals |
| Days in accounts receivable (DAR) | 45–65 days | 32–45 days | Faster ERA posting and denial resolution |
| Appeal win rate | 40–55% | 60–75% | Improved with structured appeal templates and LCD/NCD citation |
| Staff hours on denial rework (per 100 claims) | 8–12 hrs | 3–5 hrs | AI-assisted appeal drafting and auto-routing |
| Clean claim rate | 82–85% | 90–94% | Sustained improvement requires ongoing scrub rule maintenance |
Sources: HFMA Revenue Cycle Benchmark Report 2023; Clustox client composite data (anonymized, 2024–2025); AAHomecare Operational Survey 2023.
What doesn’t work yet: honest limits of DME claims processing software
- Documentation quality is still a human problem: Software can flag missing fields and route orders to a documentation hold queue. It cannot create compliant clinical documentation on the provider’s behalf. The DWO, LMN, and face-to-face encounter notes must come from qualified clinicians; software just enforces that they exist and are complete before a claim is submitted.
- Medicare Advantage plan rules drift: MA plans update their DME coverage policies annually (and sometimes mid-year). No-claims software maintains a fully current MA plan rules library for all 800+ active MA plans. Operators with high MA volume need a workflow to manually verify coverage policy changes at least quarterly.
- Complex secondary billing: Crossover claims where Medicare is primary and Medicaid is secondary still generate significant manual intervention even in fully automated setups. The 837 crossover transaction process has well-documented edge cases that most clearinghouses handle inconsistently.
- TPE and RAC audit response: Claims processing software creates the audit trail (order documentation, submission history, ERA records). It doesn’t manage the TPE or RAC response workflow itself. That requires a separate audit management process and operators facing a Targeted Probe and Educate review should not rely on their claims software alone.
- Timely filing recovery: Once a timely filing window has passed, no software can recover that claim. The only fix is a front-end process that ensures claims submit within the filing window. Medicare’s timely filing limit for DME is 12 months from date of service, per CMS MLN Matters SE0104.
Buyer’s Checklist: Evaluating Claims Processing Software For DME
Tier 1 Non-negotiables
- DME/HME-specific HCPCS scrubbing rules, not generic medical billing scrubbers adapted for DME
- Medicare Part B and Medicare Advantage claim support with payer-specific rule sets
- Native integration with your existing platform (Brightree, NikoHealth, or TIMS) no manual CSV handoffs
- Real-time or same-day 277CA acknowledgment capture you need to know immediately when a claim rejects
- 835 ERA auto-posting with exception queue for unmatched payments
- Denial reason code library mapped to recommended corrective actions (not just raw ANSI codes)
- Clearinghouse connectivity to Availity, Waystar, or Change Healthcare all three, preferably
- Audit trail and documentation storage per claim, accessible for TPE, RAC, ZPIC, and UPIC review
Tier 2 Strong differentiators
- Denial prediction scoring before submission
- AI-assisted HCPCS code and modifier suggestion
- Automated appeal letter drafting with LCD/NCD citation
- Prior authorization tracking integrated with claim workflow
- Denial pattern reporting by payer, code, and referring provider
- ACHC and BOC accreditation documentation compliance checks
Tier 3 Worth asking about
- Agentic AI workflow integration (LangGraph-based or equivalent) for complex multi-step denial resolution
- Voice or SMS patient outreach for missing documentation collection
- Predictive revenue forecasting based on payer adjudication patterns
Frequently Asked Questions
Why Do Dme Claims Get Denied At A Higher Rate Than Other Healthcare Claims?
DME claims carry a higher documentation burden than most healthcare billing every order requires a detailed written order (DWO), proof of delivery (POD), and, in many cases, a Letter of Medical Necessity (LMN). HCPCS Level II codes require correct modifier application (KX, GA, GY, GZ) and must match the payer's local coverage determination (LCD). Medicare Advantage plans maintain their own coverage rules separate from Medicare Part B, creating additional payer-rule complexity. The result: DME first-pass denial rates average 15–18%, versus 9–10% for healthcare overall, per HFMA's 2023 Revenue Cycle Benchmarking Report.
What Is The Difference Between Claim Scrubbing And Claim Editing?
Claim scrubbing is automated pre-submission validation the software checks the claim against a library of rules (HCPCS validity, modifier requirements, NPI format, and required field completion) and flags errors before the claim submits to the payer. Claim editing is the human-facing work queue where staff review and correct flagged claims. Strong claims processing software minimizes editing by catching errors at data entry, not at the scrubbing stage.
How Does Prior Authorization Affect Dme Claims Processing?
CMS expanded prior authorization requirements for certain DME categories under the Prior Authorization for Certain Hospital Outpatient Department (OPD) Services rule and subsequent expansions. For DME, prior authorization is currently required for power mobility devices, certain orthotics, and other high-utilization equipment categories. A missing or expired PA is an automatic denial. Claims processing software should track PA status per order and prevent claim submission if a required PA is not on file. For current PA requirements, reference CMS Prior Authorization and Pre-Claim Review Initiatives.
What Hcpcs Modifiers Cause The Most Dme Claim Denials?
The KX modifier is the highest-risk modifier in DME billing. KX signals that the clinical documentation meets the coverage criteria in the LCD and Medicare can audit that attestation. Incorrectly applying KX when the documentation doesn't support it risks both denial and fraud exposure. GA signals that a signed advance beneficiary notice (ABN) is on file; GY indicates the item is statutorily excluded; GZ indicates the item is expected to be denied as not medically necessary. Modifier errors applying KX without supporting documentation or using GY when GA applies are among the top correctable denial causes in DME billing.
How Long Does It Take To Fix A 15–18% Dme Claim Denial Rate?
Timeline depends on which denial categories are driving the rate. Eligibility errors and timely filing violations can be addressed within 30–60 days through workflow and software changes. HCPCS coding errors typically improve within 60–90 days with targeted training or AI-assisted coding tools. Documentation-driven denials, the largest category, at ~28% of DME denials, take the longest: 90–180 days because they require process changes with referring providers, clinical staff, and intake workflows. Operators who address all categories in parallel reach a 7–10% first-pass denial rate within 9–12 months.
Is Brightree The Best Dme Claims Processing Software?
Brightree is the market-share leader for mid-to-large DME suppliers, and its claims management module is mature and well-supported. Whether it's the right platform depends on your operation size, payer mix, and whether you plan to add an AI layer. NikoHealth is a strong alternative for cloud-native operations that want a cleaner API surface for automation. TIMS Medical is common among smaller operators and has a lower implementation cost. The 'best' platform is the one your billing staff can operate well and that your IT team can integrate with automation tools not necessarily the one with the most features.
What Is The Roi Of Improving Claims Processing For A Dme Supplier?
For a DME supplier submitting 400 claims per month at an average reimbursement of $350 per claim, reducing the denial rate from 17% to 8% recovers approximately $12,600 in previously denied revenue per month $151,200 annually before accounting for reduced rework costs. At $118 per denied claim in rework and write-off cost (HFMA), cutting 36 denials per month saves an additional $4,248/month in operational cost. Combined, the revenue and cost benefit typically exceeds the software and implementation cost within 6–12 months. AAHomecare's operational benchmarking data supports similar ROI projections for mid-size DME operators.
The bottom line: a 15–18% denial rate is not a ceiling
DME claim denials are expensive, demoralizing, and for the majority of operators largely preventable. The industry average of 15–18% persists not because the problems are unsolvable, but because most DME operations are working with billing software that was built to process claims, not to prevent denials.
The data is consistent: operators who close the workflow gaps automated eligibility verification, HCPCS code intelligence, prior auth tracking, structured claim scrubbing reach first-pass clean claim rates of 90–94% within 9–12 months. That is not a marketing projection. It is the documented outcome when the root causes are addressed systematically rather than managed reactively.
Here is what that looks like in practice for a mid-size DME supplier:
- Denial rate drops from 17% to 8–9%, recovering $100,000+ in previously denied annual revenue for a 400-claim-per-month operation
- Staff hours on denial rework cut by 50–60%, freeing billing coordinators for higher-value work instead of appeal queues
- Days in accounts receivable falls 15–20 days improving cash flow without adding headcount
- Appeal win rate climbs to 60–75% because structured appeal templates with LCD/NCD citations outperform handwritten letters every time
The starting point is not a platform switch. For most DME operators, the starting point is a clear-eyed audit of which denial categories are actually driving the rate because the fix for a documentation problem is different from the fix for an eligibility problem, which is different again from a coding problem. Get the diagnosis right first, then match the solution to the root cause.
If you want that diagnosis done in 48 hours, a workflow mapped, denial root causes quantified, and ROI modeled against your actual claim volume, that is exactly what is built to deliver. Fixed price. DME-specific. No consulting engagement required to get the answer.
Disclaimer
This article is intended for DME providers, billing managers, and operations leaders. The financial and operational benchmarks presented are estimates based on industry data and provider-reported results. Actual outcomes vary depending on payer mix, staff workflow, and software configuration.