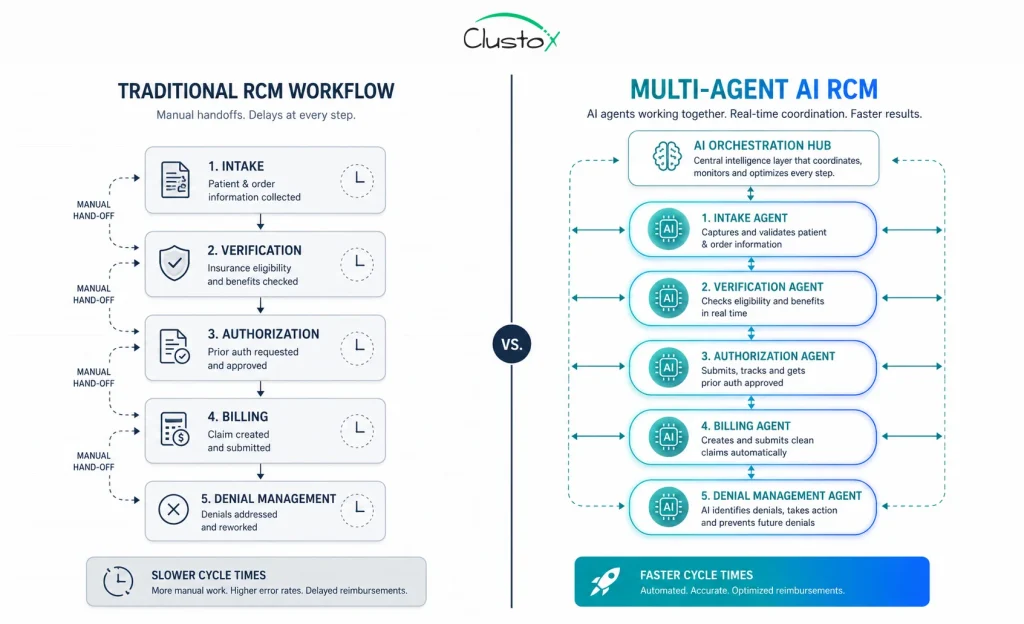
Revenue cycle operations in DME are under pressure from every direction. Payer rules change quarterly. Staff turnover is high. Prior authorization timelines stretch for days while patients wait and equipment sits idle. Denial rates climb, and each rework cycle costs your billing team time they do not have.
This is not a software problem. It is a coordination problem. And that is exactly what agentic AI operations are built to solve.
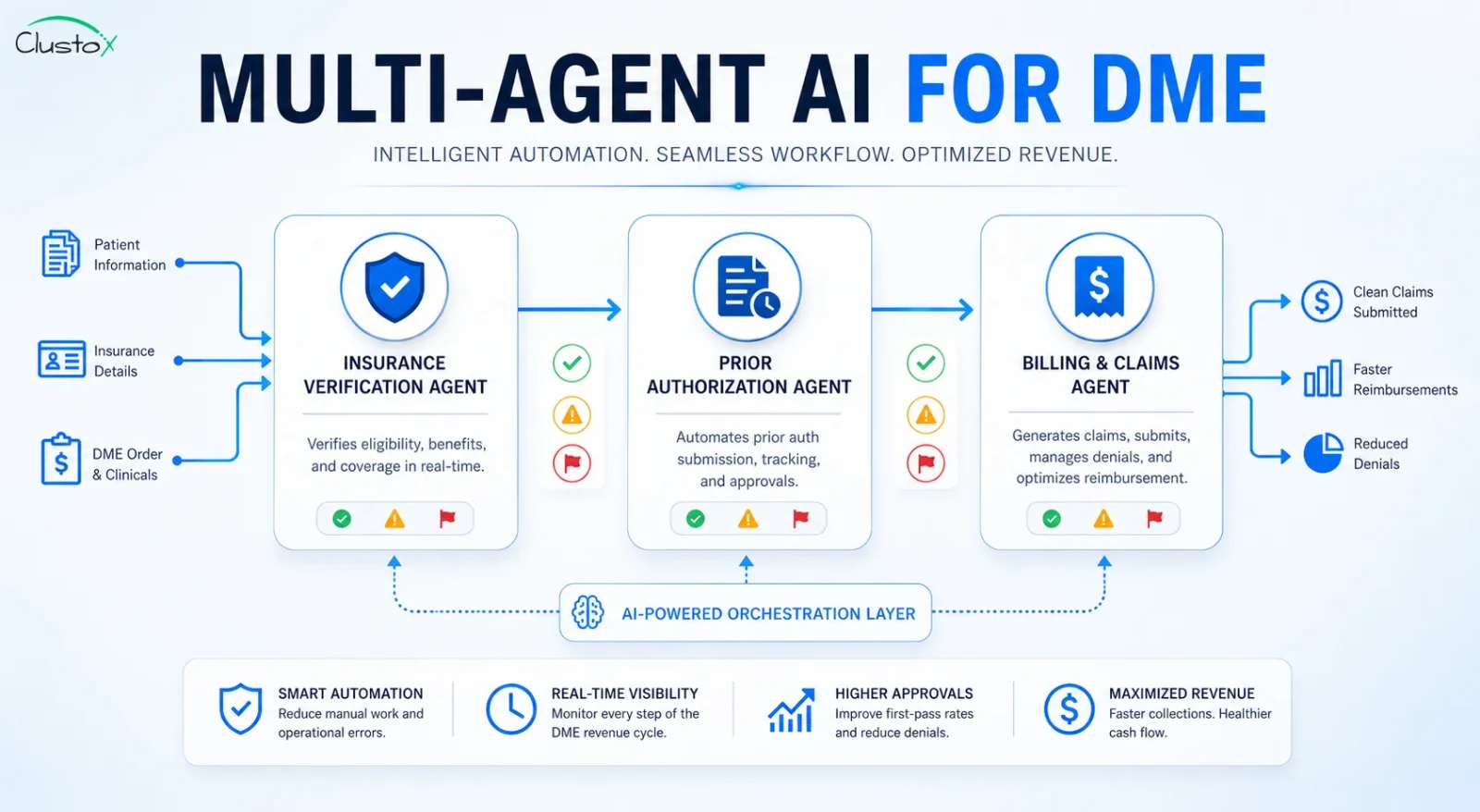
Multi-agent AI does not replace your existing workflows in one sweeping overhaul. It assigns specialized AI agents to discrete tasks such as eligibility verification, prior auth submission, and claims processing, and then coordinates them so each step feeds the next without a human having to move the handoff manually.
This guide breaks down how that coordination works, what it handles across the three core revenue cycle functions, and what you need to evaluate before deploying it inside a DME operation.
What Is Agentic AI, and Why Does It Matter for DME Revenue Cycle?
Before getting into the architecture, it helps to be clear about what agentic AI actually means in this context, because the term gets used loosely.
Most AI tools in DME right now operate as single-task assistants. They check one thing, flag one issue, or fill one field. They do not coordinate with other systems. They do not take follow-up actions. They wait for a human to review and move the work forward.
Agentic AI operations work differently. An AI agent is a system that can receive a goal, break it into steps, call the tools it needs (your payer portals, your Brightree or NikoHealth instance, your clearinghouse), and complete those steps in sequence without waiting for a human to do each handoff.
A multi-agent system takes this further. Multiple specialized agents run in parallel or in sequence, each owning a specific part of the workflow. One agent verifies eligibility. Another handles prior auth. A third monitors claims status and routes denials. A coordinating layer ties them together.
Table of Contents
This architecture matters for DME specifically because your revenue cycle is not a single linear process. It involves payer-specific rules, documentation requirements, and multiple external systems that do not talk to each other natively. A single agent cannot reliably handle all of that. Specialized agents, working in coordination, can.
How Does an AI Agent Handle Insurance Verification in DME?
Insurance verification is often the first bottleneck in your revenue cycle. It is also one of the most automatable steps, because the inputs are structured and the payer portals follow predictable patterns.
Here is what a verification agent does in practice.
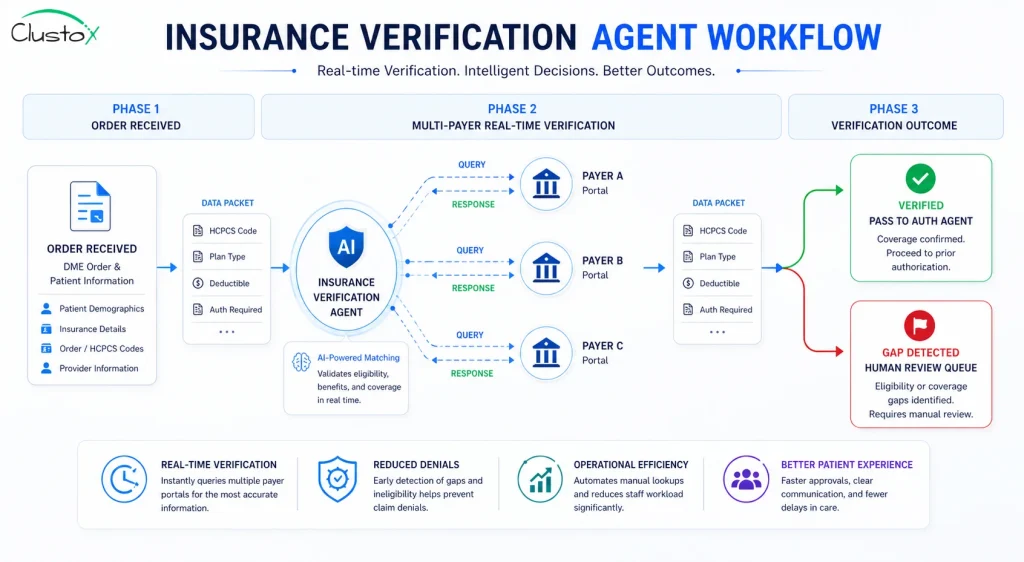
Real-time eligibility checks across multiple payers
When a new order comes in, the verification agent pulls the patient’s insurance information from your DME management system, whether that is Brightree, NikoHealth, or another platform. It then queries the relevant payer portals or runs an EDI 270/271 eligibility transaction through your clearinghouse.
It checks coverage status, deductible balances, coinsurance, and plan-specific benefit limits for the equipment category. It does not wait for a staff member to log in, navigate to the right portal, and manually pull each field.
What this changes for you: verification that takes a billing specialist 15 to 25 minutes per order can be completed in under two minutes at scale.
Flagging coverage gaps before equipment ships
The agent does not just confirm active coverage. It evaluates the data against the specific HCPCS codes on the order. It checks for prior authorization requirements tied to those codes and flags any coverage gaps, coordination of benefits issues, or plan-specific documentation requirements before the order moves forward.
This is the part that eliminates a significant share of downstream denials. Most denials at the claims stage originate from a verification gap at intake. Catching those gaps earlier means fewer write-offs later.
Passing structured data to the auth agent
Once verification is complete, the agent does not just log results in a note field. It passes structured data to the next agent in the pipeline: coverage confirmed, auth required, payer ID, plan type, and relevant documentation flags. The authorization agent picks that up and begins the prior auth process without waiting for a human review step.
This handoff is what distinguishes agentic AI from standard automation. The agents share context, not just outputs.
How Does Multi-Agent AI Manage Prior Authorization for DME?
Prior authorization is where most DME operations spend the most manual effort and where agentic AI delivers the highest return. The process involves multiple systems, payer-specific rules, and documentation requirements that change frequently.
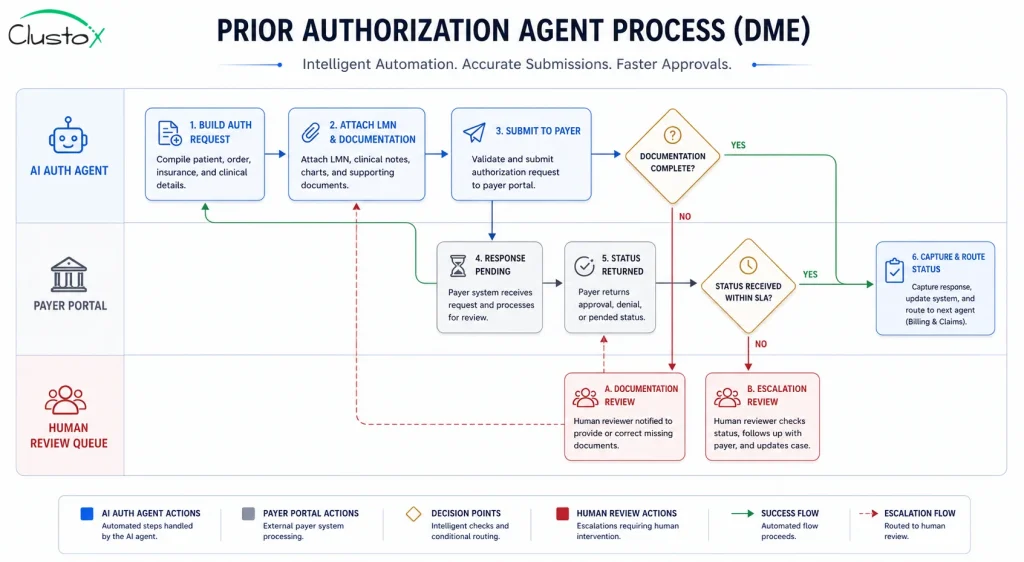
Building and submitting the auth request
The auth agent receives the structured handoff from the verification agent. It already knows the payer, the HCPCS codes, and what documentation is required. It pulls the relevant clinical documentation from your system, including the Letter of Medical Necessity (LMN), physician notes, and any supporting clinical records.
It then formats the submission according to payer-specific requirements. Different payers want different formats, different attachments, and different submission channels. The auth agent handles those variations without your team having to maintain a manual payer-by-payer knowledge base.
Monitoring submission status and following up
After submission, the agent does not just log a ‘submitted’ status and wait. It monitors the payer portal for status updates at defined intervals. If a response has not come back within the payer’s published turnaround time, the agent flags the submission and, depending on your configuration, triggers a follow-up or routes it to a specialist.
This removes the task of manually tracking hundreds of open auth requests from your team’s daily workload. The agent surfaces only the cases that need human attention.
Handling payer-specific documentation rules
This is where the operational value becomes tangible. Payers often have documentation requirements that are not published clearly or that change between plan years. A well-configured auth agent maintains a knowledge base of payer-specific rules and flags submissions that are likely to be returned for missing documentation before they are submitted.
That proactive flagging reduces the back-and-forth cycle with payers, which is one of the primary reasons prior auth timelines drag out.
How Does the Billing Agent Coordinate With Verification and Auth?
The billing agent is the third node in the pipeline, and its effectiveness depends entirely on the quality of what the verification and auth agents pass to it. This is the coordination model in practice.
Claims generation from structured upstream data
When the auth agent confirms an approval, that approval data moves to the billing agent with all relevant fields already structured: payer ID, auth number, approved HCPCS codes, approval date, and any payer conditions. The billing agent uses this data to generate a clean claim.
Because the claim is built from structured, verified data rather than from a billing specialist manually re-entering information from multiple screens, the risk of keying errors drops significantly. That matters because claim errors are one of the top reasons for initial denial.
Claim scrubbing before submission
Before the claim goes to the clearinghouse, the billing agent runs it through a scrubbing process. It checks for code pairing errors, missing modifiers, date-of-service alignment, and payer-specific billing rules. Issues that would cause a rejection are caught before submission.
This step is not new to DME billing. What is different with an AI agent is that the scrubbing rules can be updated dynamically as payer requirements change, and the agent can apply those updates at scale across every claim in the queue rather than waiting for a team training session.
Denial routing and rework coordination
When a claim is denied, the billing agent does not just log the denial code. It reads the Explanation of Benefits (EOB) or remittance data, categorizes the denial by type (clinical, administrative, coding, duplicate), and routes it to the appropriate rework path.
Administrative denials with straightforward fixes can be corrected and resubmitted by the agent. Clinical denials that require physician input or additional documentation are routed to the appropriate human with the context they need already assembled.
This triage function is one of the highest-value outputs of a multi-agent system in DME billing because it replaces the time a billing specialist would otherwise spend reading EOBs and deciding what to do with each one.
The table below summarizes how each agent in the pipeline contributes to the overall revenue cycle outcome.
| Agent | Primary Function | Upstream Input | Downstream Output |
|---|---|---|---|
| Verification Agent | Real-time eligibility check, coverage gap detection | Order data, patient insurance info | Structured coverage data, auth requirement flags |
| Auth Agent | Prior auth submission, status monitoring, documentation validation | Coverage data from Verification Agent | Auth approval data, denial flags |
| Billing Agent | Claims generation, scrubbing, submission, denial routing | Auth approval from Auth Agent | Clean claim to clearinghouse, denial rework queue |
What Does the Coordination Layer Actually Do?
The term ‘multi-agent’ only delivers value if there is a coherent coordination layer managing the agents. Without it, you have three separate automation tools that do not share context, do not hand off cleanly, and do not escalate intelligently.
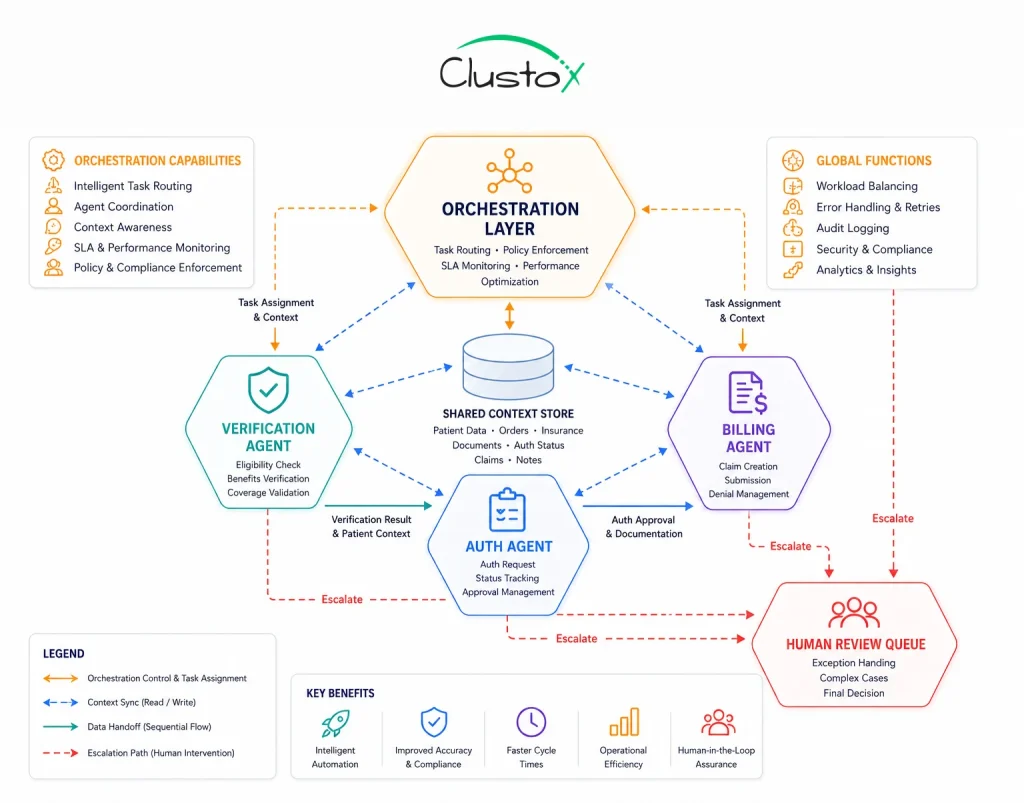
Orchestration and task sequencing
The coordination layer determines which agent acts next based on the current state of the workflow. If the verification agent returns a result that requires auth, the coordination layer routes the order to the auth agent. If auth is not required, it routes directly to billing. If the verification returns a gap that requires human review, the coordination layer holds the order and surfaces it to the right queue.
This sequencing logic is what makes the system behave like a coordinated team rather than three independent tools.
Context sharing between agents
Each agent in the pipeline needs to know what happened in the previous step. The coordination layer maintains a shared context object for each order that all agents can read and write to. This means the billing agent does not need to re-verify coverage or re-look up the auth number. It reads from the shared context and proceeds.
Context sharing also enables better exception handling. If the auth agent encounters a payer rule that conflicts with the coverage data the verification agent returned, the coordination layer can flag that conflict rather than allowing a bad claim to proceed.
Human-in-the-loop escalation
Agentic AI operations are not designed to remove humans from the revenue cycle entirely. They are designed to remove humans from the tasks that do not require human judgment. The coordination layer defines the escalation rules: what scenarios route to a billing specialist, what scenarios route to a clinical reviewer, and what scenarios require supervisor authorization.
A well-configured coordination layer means your team focuses on the 10 to 15 percent of cases that genuinely need their expertise, rather than spending 80 percent of their time on routine processing.
What Are the Real Operational Outcomes DME Providers Can Expect?
It is worth being direct about what multi-agent AI delivers and what it does not, because the expectations gap is where most AI implementations fail.
The measurable outcomes that DME providers report after deploying coordinated agentic AI operations fall into three categories.
Reduction in prior auth cycle time
CMS data shows that the average prior authorization decision takes 11 calendar days under manual processes. Providers using automated auth workflows report reducing that to two to three days in standard cases.
The reduction is not uniform across all payers or all equipment categories. Complex clinical cases still require human review. But for the majority of standard orders, the cycle time compression is real and measurable.
Lower denial rates at first submission
When verification data flows cleanly into auth, and auth approvals flow cleanly into billing, the claim that reaches the clearinghouse is built from accurate, pre-verified data. The administrative denial categories such as missing auth numbers, incorrect payer IDs, and mismatched coverage dates drop significantly.
Clinical denials are a different story. They require appropriate documentation and physician input. Agentic AI does not resolve clinical denial risk on its own. What it does is ensure that the administrative side of every claim is clean so that when a clinical denial does occur, it is a genuine clinical issue and not a data error.
Staff reallocation from processing to exceptions
The most significant operational change is where your staff spends time. A multi-agent system that handles routine verification, auth submission, and claim generation frees billing staff to focus on exceptions: complex denials, appeal submissions, payer negotiations, and the cases that genuinely require expertise.
This is not a headcount reduction argument. It is a capacity argument. The same team can handle a higher order volume without a proportional increase in headcount.
What Should You Evaluate Before Deploying Multi-Agent AI in Your DME Operation?
The architecture described above works when it is implemented against a clean operational foundation. There are several factors you need to assess before a deployment will produce reliable results.
The following table covers the key evaluation criteria and what each one means for your readiness.
| Evaluation Area | What to Assess | Why It Matters |
|---|---|---|
| Data quality | Are your patient records, insurance data, and order data clean and consistently structured in your DME system? | Agents work from the data they receive. Garbage in, garbage out applies here more than anywhere. |
| System integration | Does your DME management platform (Brightree, NikoHealth, etc.) support API access or EDI integration? | Agents need programmatic access to your systems. Manual portal access creates bottlenecks. |
| Payer portal access | Do you have stable access to the payer portals relevant to your top 10 payers by volume? | Verification and auth agents depend on reliable portal access. Frequent portal changes require ongoing maintenance. |
| Escalation design | Have you defined the scenarios that require human review, and who handles each one? | Without defined escalation paths, the coordination layer cannot route exceptions correctly. |
| Compliance posture | Are your HIPAA data handling policies in place for AI-processed patient data? | PHI flows through these agents. Your compliance requirements apply to every system in the pipeline. |
One point worth emphasizing: the agents described in this guide are tools that operate within your existing payer relationships and CMS requirements. They do not change what is billable, what requires authorization, or what documentation standards apply. They automate the execution of those requirements.
How Does This Fit With Your Existing DME Software Stack?
One of the most common concerns when evaluating agentic AI operations is integration: how does this work with Brightree, NikoHealth, TIMS, or whichever platform you run today?
The short answer is that multi-agent AI systems are designed to sit alongside your existing software, not replace it. They interact with your systems through APIs, EDI transactions, and in some cases structured web automation where APIs are not available.
Your DME management platform remains the system of record. The agents read from it, act on external systems (payer portals, clearinghouses), and write structured results back. Your billing team still works in the same interface they use today. What changes is how much of the manual queue is already worked by the time they log in.
The practical integration requirements vary by platform. Brightree, for example, has an API ecosystem that supports structured reads and writes. Other platforms may require EDI-based integration or custom connectors. A pre-deployment technical assessment is the right starting point for any DME operation considering this architecture.
What Are the Limits of Multi-Agent AI in DME Revenue Cycle?
Every serious guide on this topic has to name the limits.
Here are the ones that matter.
- Agents are only as good as the rules they are given. If your payer rule library is incomplete or outdated, the auth agent will make the same mistakes a new employee would make.
- Complex clinical cases still require human judgment. An agent can identify that a case requires physician documentation. It cannot substitute for the physician’s clinical assessment.
- Payer portal instability affects agent performance. If a payer changes its portal layout or authentication requirements, the agent’s access to that portal may break until the integration is updated.
- Implementation takes time. A multi-agent system deployed against a messy data environment will produce unreliable results. Cleanup and configuration work precede performance gains.
- HIPAA compliance responsibility stays with you. The fact that an AI agent is processing PHI does not transfer your compliance obligations. Your Business Associate Agreements and data handling policies apply to every tool in the pipeline.
How Do You Build a Business Case for Agentic AI Operations in DME?
If you are putting together an internal case for this investment, the numbers to anchor it are straightforward.
Start with your current prior auth volume per month. Multiply by the average staff hours per auth submission (typically two to four hours across the full cycle in manual operations). That is your cost baseline for auth processing.
Then look at your first-pass denial rate. A multi-agent system that reduces auth cycle time and cuts administrative denial rates has a calculable return against both of those baselines. The deployment cost, integration timeline, and ongoing maintenance should be weighed against that baseline reduction.
The goal is not to build a projection based on best-case assumptions. It is to build a conservative case based on documented current costs. That is the conversation your finance team and payer relations team will engage with.
Beyond the numbers, one factor shapes how credible that business case actually is: who builds the system. That question is worth addressing directly.
Why off-the-shelf tools fall short for DME
Generic automation platforms are built for horizontal use cases. They can handle parts of your revenue cycle workflow. But the coordination layer, the payer-specific rule sets, and the escalation design require custom engineering. A tool built for general healthcare billing does not arrive with your payer mix pre-configured, your HCPCS categories mapped, or your denial patterns already accounted for.
That gap adds months of configuration work after the sale. And in that configuration period, the system is not producing the outcomes your business case projected.
What a custom agentic AI partner changes
A partner that builds custom agentic AI systems for DME operations approaches the engagement differently. The build starts with your payer mix, your DME software stack (Brightree, NikoHealth, TIMS, or otherwise), and your specific denial patterns.
Instead of adapting a horizontal platform to fit your workflows, the system is designed around them from the start. That makes the business case numbers more defensible, because the projections are built on your actual data rather than industry averages that may not reflect your operation.
What a pre-deployment assessment should give you
Before any build begins, a qualified partner should run a structured assessment of your current workflows. That means mapping how verification, auth, and billing actually move through your operation today, not how your SOPs say they should move.
The assessment identifies where the data quality gaps are, which payer integrations are stable enough to automate against, and what the system will handle autonomously versus what will still route to a human reviewer. That output is a deployment roadmap you can take directly to your finance team. It tells you exactly what you are buying before you commit to building it.
Frequently Asked Questions (FAQs)
Does a multi-agent AI system need to replace our existing DME software?
No. Multi-agent systems are designed to integrate with platforms like Brightree, NikoHealth, and TIMS, not replace them. Your existing platform remains the system of record. The agents interact with it via API or EDI and handle the external-facing work with payer portals and clearinghouses.
How long does it take to deploy a multi-agent AI system for DME revenue cycle?
A realistic deployment timeline for a focused implementation covering verification, auth, and billing coordination is three to six months. That includes the integration build, payer rule configuration, testing against your specific payer mix, and staff onboarding. Operations with cleaner data environments and available API access tend toward the shorter end of that range.
Is patient data safe when processed by AI agents?
Your HIPAA obligations apply to every system that processes PHI, including AI agents. Any deployment should include a Business Associate Agreement with the AI vendor, a data handling review, and an assessment of how PHI is stored or transmitted during agent processing. The technology does not change your compliance responsibilities.
What prior authorization scenarios still require human review?
Complex clinical cases, appeals requiring physician attestation, and any scenario where the payer's documentation requirements exceed what your existing clinical records contain will still route to a human reviewer. The agent's role in those scenarios is to assemble the available documentation and surface the case with the relevant context, not to resolve it independently.
Can multi-agent AI handle Medicare Advantage payer variability?
Medicare Advantage plans vary significantly by plan sponsor, and their prior authorization rules are not standardized. A well-configured auth agent can maintain payer-specific rule sets for your top Medicare Advantage plans by volume. Plans with lower volume or unusual documentation requirements will require more manual oversight until sufficient case history is available to build reliable rules.
Conclusion
Multi-agent AI for DME revenue cycle is not a future-state concept. DME providers are deploying it today against real payer workflows, real authorization requirements, and real billing pipelines.
The coordination model described in this guide, verification feeding auth, and auth feeding billing, with a shared context layer and defined human escalation paths, are the architecture that makes agentic AI operations reliable in a complex regulatory environment like DME.
The operational gains are real: shorter auth cycles, fewer administrative denials, and a billing team that spends its time on exceptions rather than routine processing. The limits are also real, and any deployment that ignores them will underperform.
If your operation is processing more than 200 orders per month and your team is spending significant time on manual auth follow-up and denial rework, the business case for a multi-agent system is almost certainly there. The question is not whether the technology works. The question is whether your data, your integrations, and your escalation design are ready for it.
Want to audit your DME revenue cycle for agentic AI readiness?
Clustox builds custom agentic AI that coordinates your verification, auth, and billing end-to-end. The build starts with your payer mix and your data, not a generic template
This article is intended for DME providers, operations leaders, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, accreditation standards) are accurate as of the review date; regulations change frequently and providers should consult primary sources or qualified counsel for current requirements.