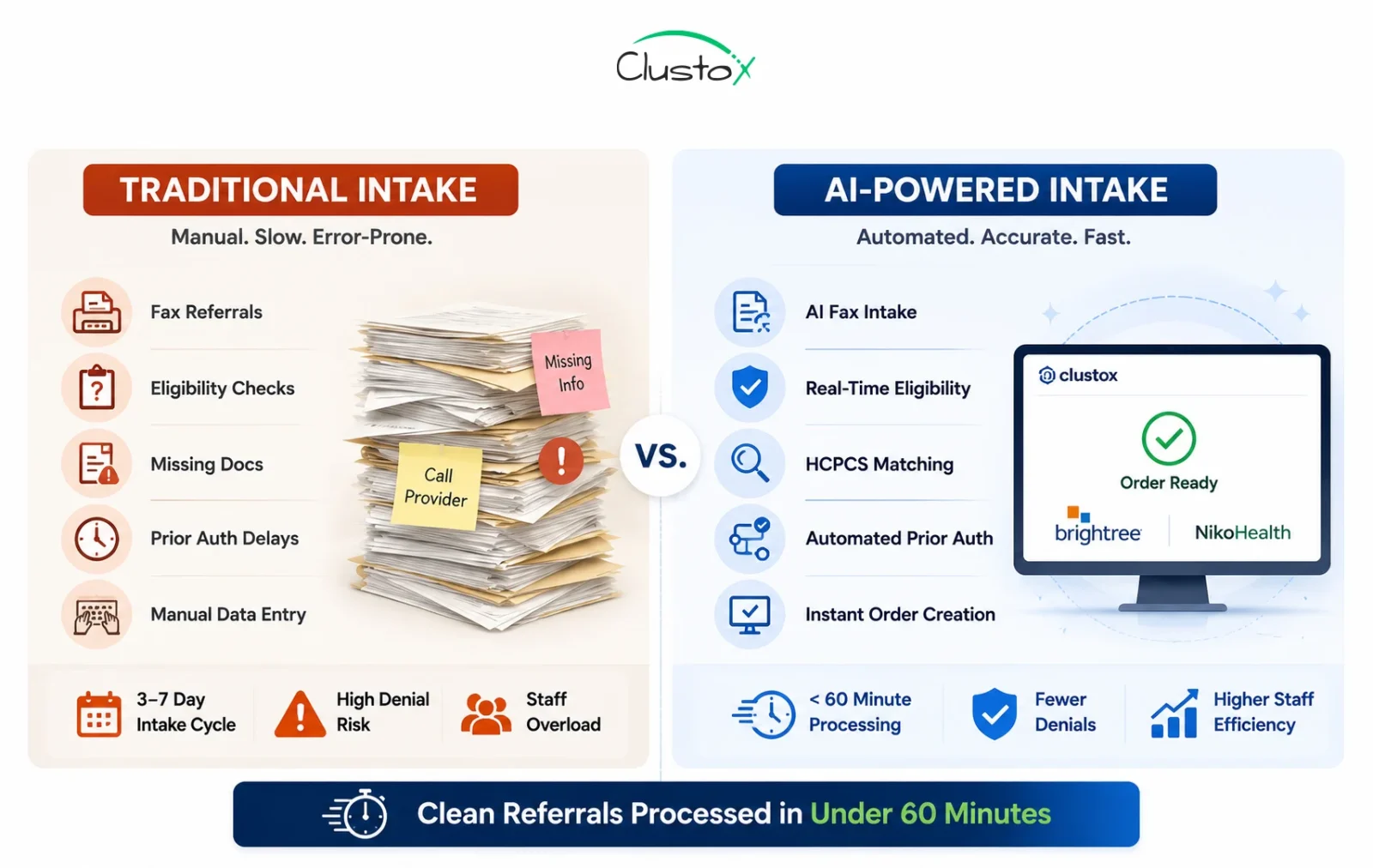
Most DME providers still process new patient orders the same way they did a decade ago: a fax lands on someone’s desk, a coordinator keys data into systems like Brightree or NikoHealth by hand, eligibility is checked through separate payer portals, and staff spend hours chasing missing documentation from physician offices.
The result is a 3–7 day intake cycle that delays patient care, drains staff capacity, and erodes already-tight margins.
Modern Agentic AI-powered patient intake software compresses this cycle by automating document ingestion, eligibility verification, HCPCS code matching, and prior authorization routing without requiring you to replace your existing systems.
In this guide, you’ll learn how Agentic AI-powered patient intake software transforms this entire workflow from fax intake to eligibility verification, HCPCS code matching, and prior authorization, reducing turnaround time to under 60 minutes without replacing your existing systems.
What This Article Covers
- Why traditional DME intake workflows break down and what they cost operators
- How Agentic AI-powered intake software automates the full referral-to-approval sequence
- The five specific workflow steps from fax ingestion to payer submission
- Prerequisites and integration requirements for Brightree, NikoHealth, and TIMS
- Real performance benchmarks from DME operations running automated intake
- Where current tools fall short and what to watch for in vendor evaluations
- A practical buyer’s checklist for assessing intake automation vendors
Why Is Traditional DME Patient Intake So Broken?
DME intake sits at the intersection of three systems that were never designed to work together: the referral source (physician offices or hospital discharge planners), the payer (Medicare, Medicare Advantage, Medicaid, or commercial insurance), and the provider’s internal platform (Brightree, NikoHealth, TIMS, or similar).
Every handoff between those systems is still largely manual, and every manual touchpoint introduces delays, errors, and unnecessary labor costs.
A typical incoming referral forces intake coordinators to move through a long chain of repetitive administrative tasks. They must sort and classify incoming faxes, verify patient demographics against payer records, run eligibility and benefits checks, and confirm HCPCS code coverage under the patient’s specific insurance plan.
Table of Contents
From there, the process becomes even more fragmented, determining whether prior authorization is required, identifying missing documentation, and following up on critical paperwork such as physician notes, Letters of Medical Necessity (LMNs), and supporting clinical evidence.
This work is not intellectually difficult, but it is highly manual, repetitive, and extremely vulnerable to human error when handled at scale. According to AAHomecare’s 2024 HME Regulatory Priorities, documentation errors during intake are consistently ranked among the top three causes of DME claim denials, alongside eligibility mismatches and missing prior authorizations.
The operational burden grows quickly with volume. Intake coordinators often process between 25 and 40 referrals per day, with each referral requiring anywhere from 20 to 45 minutes of active work. As referral counts increase, labor costs rise proportionally, while delays in collecting documentation slow both patient onboarding and reimbursement cycles.
The result is a workflow that creates friction at every stage of the revenue cycle. Claims are delayed or denied, staff spend additional hours on rework and appeals, and patients are left waiting longer for confirmation and equipment delivery. In a market where speed, accuracy, and compliance directly impact both revenue and patient satisfaction, traditional DME intake has become one of the largest operational bottlenecks for providers today.
What Is DME Patient Intake Software and How Does It Actually Work?
DME patient intake software is a workflow automation layer that sits between your referral sources and your order management system. In its Agentic AI form, it does not simply route documents from one inbox to another.
It reads incoming referrals, extracts structured data, validates that data against payer rules and internal formularies, identifies documentation gaps, and takes action to resolve those gaps before a human coordinator ever touches the order.
The intake sequence for a well-configured Agentic AI system follows 5 steps:
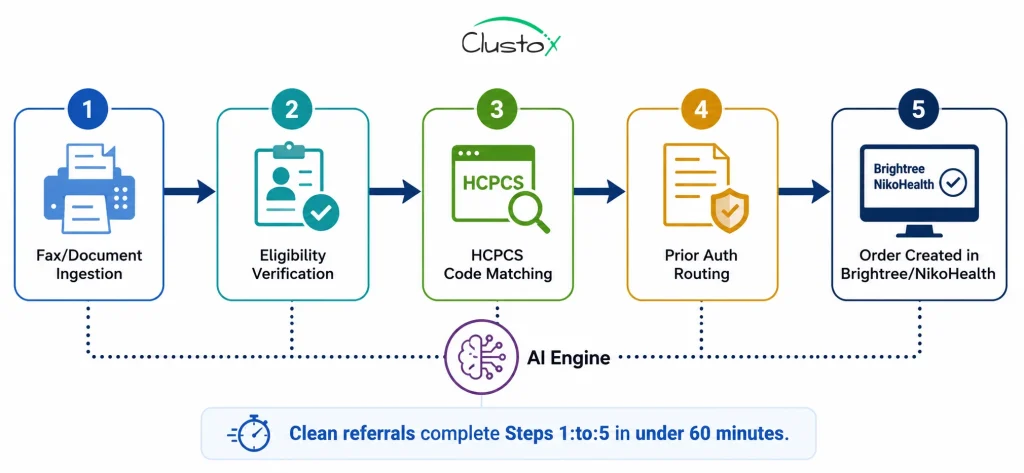
Step 1: Document Ingestion
The system captures faxes via digital fax integration or eFax API, intake forms submitted through a patient or referral web portal, and orders routed from hospital EHR systems. An LLM-based extraction layer reads unstructured documents and pulls out patient demographics, referring physician NPI, ICD-10 diagnosis codes, requested equipment type, and any attached clinical notes.
Tools like AWS Bedrock with a RAG (retrieval-augmented generation) layer allow the system to match extracted equipment descriptions to the correct HCPCS codes even when the prescriber uses informal terminology instead of precise billing language.
Step 2: Real-Time Eligibility and Benefits Verification
Once patient data is extracted, the system queries payer eligibility in real time using the patient’s payer ID, date of birth, and member number. This replaces the manual portal check that coordinators run one payer at a time.
For patients covered by Medicare Advantage or commercial plans layered over Medicare, the system checks primary and secondary benefits simultaneously and flags any coordination-of-benefits conflicts for human review.
Step 3: HCPCS Code Matching and Documentation Requirements
The system cross-references the requested equipment against the correct HCPCS code and retrieves the documentation requirements for that code under the applicable payer. For a CPAP device (E0601), for example, the system checks whether a qualifying sleep study result is attached and whether the treating physician’s LMN meets CMS Local Coverage Determination (LCD) criteria.
If documentation is incomplete, the system flags the specific gap and either sends an automated request to the referral source or queues the item for coordinator follow-up.
Step 4: Prior Authorization Routing
Where the HCPCS code and payer combination requires prior authorization, the system initiates the PA request automatically.
It pre-populates the authorization form with extracted clinical data and submits it to the payer portal or clearinghouse. For payers that accept electronic prior authorization via X12 278 transactions, end-to-end submission happens without coordinator involvement.
Step 5: Order Creation in the DME System
Once eligibility is confirmed and authorization is initiated, the system creates the order record in Brightree, NikoHealth, or TIMS, including all relevant codes, payer information, and documentation attachments. The coordinator receives a complete, validated order rather than a raw fax requiring manual processing.
How Does AI Intake Software Integrate With Brightree and NikoHealth?
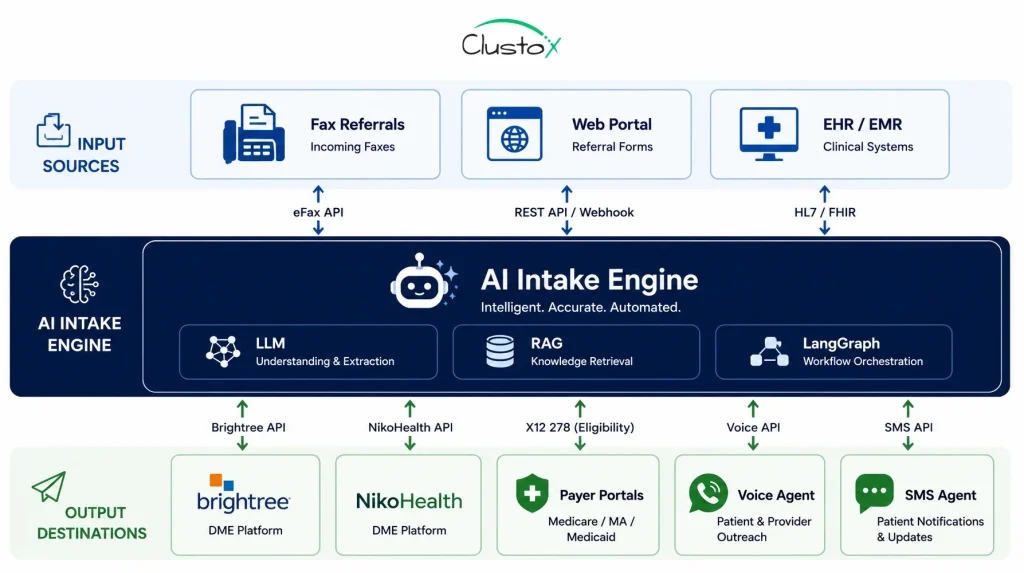
Brightree and NikoHealth both expose API endpoints that allow third-party intake automation tools to create and update order records without manual data entry. For Brightree, integration typically uses the Brightree API to write patient demographics, order details, insurance information, and documentation attachments directly into a new order record.
NikoHealth’s architecture, being API-first from inception, generally supports tighter integration with less configuration overhead.
The integration pattern that works best for most DME providers uses a middleware layer: the intake AI handles extraction, validation, and payer communication, then writes a completed, validated order into the DME platform.
Your existing Brightree or NikoHealth workflows downstream (delivery scheduling, billing, and collections) remain entirely unchanged. The automation eliminates the manual data entry that happens before the order exists, not the work that happens after.
For DMEs running TIMS or Universal Software Solutions, integration complexity increases because those platforms have less modern API infrastructure.
Intake AI vendors typically handle these systems with an RPA (robotic process automation) layer, which functions reliably but introduces additional points of failure that require monitoring.
Voice agents and SMS agents built on LangGraph-based architectures extend the intake workflow outward: calling referral sources to confirm missing documentation, texting patients to complete intake forms, and following up on outstanding LMNs.
These outbound touchpoints are particularly valuable for cutting the document chase cycle that commonly stalls intake between 24 and 72 hours.
What Does Implementation Actually Require for DME Providers?
Most DME providers can go live with an intake automation system in 6 to 12 weeks if the following prerequisites are in place before the engagement begins. Providers who skip this readiness work typically experience longer timelines and more configuration iterations.
1. Technical Prerequisites
- Active Brightree, NikoHealth, or TIMS account with API access enabled. Brightree API access requires a formal support request and may carry additional fees depending on your contract tier.
- A digital fax solution or eFax integration. Traditional physical fax infrastructure requires an additional conversion layer and introduces image quality variability that degrades document extraction accuracy.
- Payer enrollment for electronic eligibility transactions (270/271) if not already active. Most mid-size DME providers have this in place; smaller operations may need to enroll through their clearinghouse.
- Secure, HIPAA-compliant document storage with a Business Associate Agreement in place with any cloud storage provider in the data path.
2. Operational Prerequisites
- A documented intake workflow showing your current steps, systems, decision rules, and escalation paths. The AI system needs to replicate your logic, not a generic template.
- A payer matrix listing every payer you bill, the HCPCS codes you use most frequently, and which payer-code combinations require prior authorization.
- A named coordinator or operations lead who owns the integration during rollout and serves as the primary escalation contact for edge cases that the system cannot resolve independently.
3. HIPAA Architecture Considerations
Any intake software handling Protected Health Information (PHI) must operate within a HIPAA-compliant architecture. Requirements include Business Associate Agreements with all vendors in the data path, data encryption in transit (TLS 1.2 or higher) and at rest (AES-256), role-based access controls with audit logging, and documented breach notification procedures.
CMS and HHS maintain current HIPAA Security Rule guidance at HHS.gov. ACHC and BOC accreditation standards also require documented data security policies for DME providers, so verify compliance posture before signing any vendor agreement.
4. Implementation Timeline
A realistic go-live sequence looks like this: document ingestion and eligibility automation go live in weeks 2 to 4. HCPCS code matching and documentation gap detection follow in weeks 4 to 8; prior authorization routing is typically last, in weeks 8 to 12, because PA workflows vary significantly by payer and require the most per-payer configuration work.
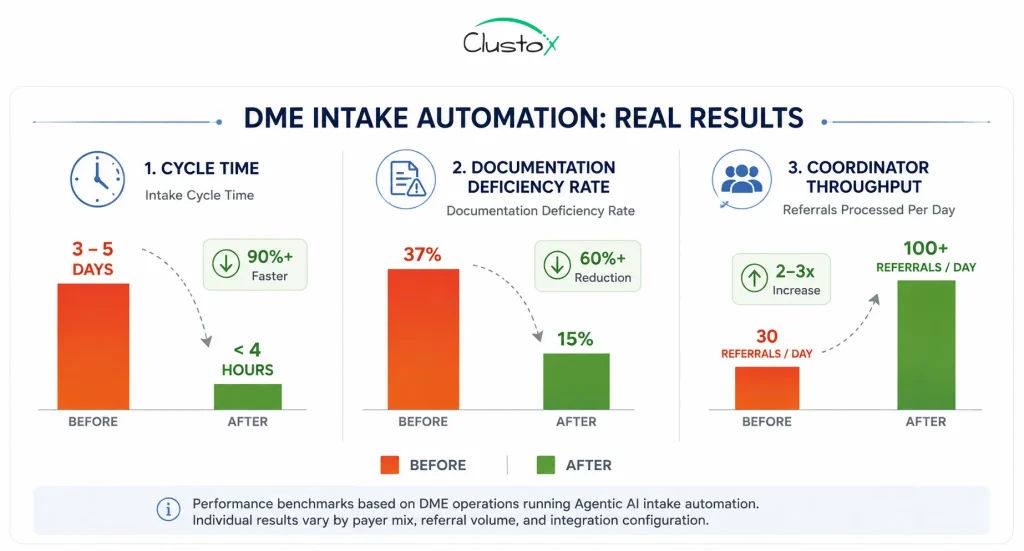
What Real Numbers Are DME Providers Seeing With Intake Automation?
Performance benchmarks from DME operations running Agentic AI intake automation show consistent, measurable improvement across the metrics that matter most to operations and billing leadership.
| Metric | Manual Workflow | With AI Automation |
|---|---|---|
| Clean referral cycle time | 3 to 5 business days | Under 4 hours |
| Prior auth initiation lag | 24 to 48 hours post-receipt | Under 15 minutes |
| Documentation deficiency rate | 30 to 45% of referrals | 12 to 18% of referrals |
| Coordinator throughput (per day) | 25 to 40 referrals/FTE | 80:120 referrals/FTE |
| First-pass denial rate reduction | Baseline | 15 to 30% improvement |
A 2023 HFMA report found that healthcare providers who automated front-end revenue cycle functions, including eligibility and prior authorization, reduced claim denial rates by an average of 22% within the first year. Source: HFMA Revenue Cycle Automation Report (2023)
CMS data shows that prior authorization requests for DME that are submitted electronically are processed on average 4.7 times faster than those submitted by phone or fax. Source: CMS Prior Authorization Final Rule for DME (2024)
Clean referrals with a complete documentation process in under 4 hours with well-configured automation, compared to 3 to 5 business days manually. Referrals requiring prior authorization drop from 6 to 10 days to 1 to 2 days because the system initiates the PA request immediately on referral receipt rather than waiting for coordinator availability.
Documentation deficiency rates on first submission drop from 30% to 45% to 12% to 18% because the system identifies missing items at ingestion, not during billing review.
These are operational gains, not technology benchmarks. The tangible results are faster patient access to equipment, fewer denial cycles, and coordinators freed to focus on complex cases that genuinely require human judgment.
What are the Current Limits of DME Intake Automation?
Intake automation reduces manual work significantly, but it is not a complete replacement for experienced intake coordinators. The gaps are real, and understanding them helps set accurate expectations and design appropriate fallback workflows.
1. Complex or Atypical Insurance Situations
Patients with multiple active insurance policies, Medicare Advantage plans with non-standard formularies, or Medicaid managed care organizations that deviate from standard CMS LCD criteria require human review. Automated eligibility checks follow standard benefit structures well. They do not reliably catch edge cases such as coordination-of-benefits errors, plan-level carve-outs, or benefits that have been exhausted mid-year.
2. Low-Quality or Non-Standard Referral Documents
LLM-based document extraction performs well on typed or digitally generated referral forms. Accuracy degrades on handwritten physician notes, faxes with poor image resolution, and non-standard order formats from small or rural practices. Plan for a 5% to 15% document exception rate and design a coordinator fallback workflow that can pick up at the point of failure without restarting the entire process.
3. Payer Portal Variability
Prior authorization submission automation works reliably for large national payers that support electronic PA via standard X12 278 transactions or modern API integrations. It works poorly for smaller regional Medicaid managed care organizations and Medicare Advantage plans with proprietary portal requirements. These payers often require phone-based PA submission or portal interactions that are difficult to automate at this point in the technology cycle.
4. HCPCS and LCD Code Maintenance
CMS updates HCPCS codes and LCD coverage criteria periodically. A system configured correctly for E1390 (oxygen concentrator) criteria in 2025 may not reflect 2026 LCD changes without a vendor-pushed update. Ask every vendor directly how they manage code and coverage updates, who owns that responsibility contractually, and what the notification process looks like when changes are applied.
5. Audit Exposure From Speed
Automated intake that moves faster than human review can inadvertently increase audit risk if speed comes at the expense of documentation quality. CMS TPE (Targeted Probe and Educate), RAC, and ZPIC/UPIC audit programs all scrutinize DME documentation completeness closely. Any intake automation system should include positive documentation completeness scoring: not just gap detection, but a confirmed check that documentation meets LCD requirements before the order is created and the claim is eventually submitted.
The OIG identified DME as a consistently high-risk area for Medicare fraud and documentation errors, with TPE audits recovering over $2 billion in improper payments between 2016 and 2023. Source: OIG Work Plan: DME Audits (2023)
Buyer’s Checklist: How Should DME Operators Evaluate Intake Software?
Use the following criteria when assessing intake automation vendors. The goal is not to find a system with the longest feature list, but to find one whose capabilities align with your actual payer mix, referral volume, and integration environment.
| Evaluation Criterion | What to Ask and Verify |
|---|---|
| System Integration | Does the vendor support native API integration with Brightree, NikoHealth, or TIMS? Native API is more stable and auditable than RPA/screen-scraping alternatives. |
| Payer Coverage | What percentage of your payer mix is supported for real-time eligibility (270/271) and electronic prior authorization (X12 278)? Request a specific list. |
| Document Extraction Accuracy | What is the vendor's documented extraction accuracy rate on fax-originated referrals? Ask for exception rate data and what triggers human review. |
| HCPCS and LCD Logic Maintenance | Who is responsible for keeping HCPCS code coverage criteria and LCD updates current, and how frequently are they applied? |
| HIPAA Architecture and BAA | Does the vendor provide a Business Associate Agreement? Ask for their most recent SOC 2 Type II report and confirm all PHI handling is documented. |
| Exception Handling Workflow | What happens when the system cannot resolve an intake issue automatically? Is there a clear coordinator escalation queue with context included? |
| Audit Trail and Logging | Does the system maintain a complete, timestamped log of every action on a referral? Non-negotiable for TPE, RAC, and ZPIC audit defense. |
| Reporting and ROI Measurement | Does the vendor provide operational reporting so you can measure cycle time, deficiency rates, and throughput before and after go-live? |
Frequently Asked Questions
How long does DME patient intake take with automation in place?
Clean referrals with complete documentation can be processed in under 60 minutes with a well-configured intake system. Referrals requiring prior authorization typically complete in 1 to 2 business days, compared to 6 to 10 days with manual workflows, because the system initiates the PA request within minutes of referral receipt rather than waiting for a coordinator to have capacity.
Does intake automation work with Medicare and Medicare Advantage plans?
Yes, with important differences between the two. Traditional Medicare (fee-for-service) is well-supported because eligibility queries via 270/271 transactions and prior authorization via X12 278 follow CMS-defined standards. Medicare Advantage plans present more variability because each plan sets its own formulary, PA requirements, and coverage criteria. Most intake automation systems support the major national MA carriers. Smaller or regional MA plans may require manual handling for PA submission.
Is DME intake automation HIPAA-compliant?
Compliance depends on implementation, not software category. Any vendor handling PHI must operate under a signed Business Associate Agreement and must maintain technical safeguards required by the HIPAA Security Rule (45 CFR Part 164). Providers remain responsible for their own compliance posture regardless of vendor claims. Review current HHS guidance directly at HHS.gov and verify BAA terms with every vendor in your data path before signing any agreement.
Will intake automation integrate with our existing Brightree setup?
Most intake automation platforms support Brightree integration via the Brightree API, writing order records, insurance information, and documentation attachments directly into a new order shell without manual data entry. API access may require a formal request to Brightree support and could incur additional costs depending on your contract. Confirm API availability and associated fees with Brightree before committing to a vendor that relies on it.
What HCPCS codes does intake automation typically cover?
Most systems cover high-volume DME categories, including CPAP and respiratory equipment (E0601, E0470, E1390), power wheelchairs and mobility aids (K0800:K0899 series), enteral nutrition (B4000 series), and hospital beds (E0250:E0304). Less common codes may require manual configuration. Always request a specific list of supported codes from any vendor, and ask how new codes or LCD changes are added to the system after go-live.
What happens when the system cannot process a referral automatically?
Any well-designed intake system routes exceptions to a coordinator queue with a clear summary of what was attempted and why automatic processing failed. The coordinator picks up from the point of failure rather than starting the referral over from scratch. Exception rates typically run between 5% and 20% of total referral volume, depending on document quality, payer mix complexity, and how well the system is configured for your specific workflows.
How does intake automation affect claim denial rates?
Intake automation addresses the upstream causes of denials: documentation gaps, eligibility mismatches, and HCPCS code errors that are identified before the order is created rather than surfaced during claims adjudication. DME providers report first-pass denial rate reductions of 15:to:30% after implementing intake automation. Importantly, intake automation does not address post-submission denial causes such as medical necessity disputes, TPE audit selections, or coordination-of-benefits errors discovered after the claim is paid.
How much does DME patient intake automation typically cost?
Most enterprise intake systems are priced per referral processed (typically $3:to:12 per referral depending on included services) or as a platform subscription with volume tiers. At 500 referrals per month, a $7:per:referral model represents $3,500 per month. Compare that against the fully loaded cost of the coordinator capacity the automation offsets, which typically runs 0.5:to:1.0 FTE. Request a vendor-prepared ROI projection based on your actual referral volume, HCPCS mix, and payer distribution before making a decision.
Can intake automation handle CPAP resupply orders as well as new patient intake?
Ongoing CPAP resupply (E0601 and supply codes A7030:A7046) can be partially automated, but resupply has different workflow requirements from new patient intake. Re-supply automation typically involves outbound SMS or voice agent outreach to existing patients to confirm continued equipment need and gather compliance data (e.g., device usage hours), followed by automated order creation based on the established re-supply schedule. This is generally configured as a separate module from new patient intake.
Bottom Line
DME patient intake is one of the highest-leverage workflows for operational automation because it is high-volume, rules-based, repetitive, and directly upstream of your revenue cycle. An Agentic AI intake system that compresses a 4-day cycle to under 4 hours for clean referrals is not a technology experiment. It is an operational investment with a measurable return in coordinator capacity, denial reduction, and patient throughput.
The performance gap between DME providers who automate intake and those who do not will widen as competitive bidding pressure continues to compress margins and as CMS prior authorization requirements expand to additional equipment categories. Providers who can confirm a referral, verify eligibility, and initiate prior authorization in under 60 minutes will consistently capture patients that slower competitors lose to the abandonment window.
Implementation takes preparation and a realistic 6-to-12-week timeline, and the technology has genuine limits around complex insurance situations and non-standard documents. For DME operations processing 200 or more referrals per month; however, the operational case is clear. If you want to understand exactly where automation applies to your specific workflow, an AI Readiness Audit produces a workflow map and ROI model tailored to your environment.
Ready to Map Your DME Intake Opportunity?
Clustox helps DME providers identify automation opportunities across prior authorization, eligibility verification, and intake workflows.