Administrative work is swallowing DME operations. Prior authorization alone consumes an average of 6 to 9 days per complex order. Eligibility verification errors drive a significant share of soft denials. Patient intake requires 45 to 60 minutes of staff time per new patient.
Denial management adds hours of follow-up work on claims that could have been prevented or automatically appealed. Multiply those hours across hundreds of orders per month, and the picture becomes clear: administration is not a background cost. It is the primary constraint on how much revenue a DME operation can process with a given headcount.
The operators gaining ground in 2026 are not hiring their way out of this constraint. They are automating the workflows that have always been manual, not with basic rules-based tools, but with Agentic AI systems that can navigate payer portals, verify eligibility in real time, classify and appeal denials automatically, and run patient outreach through voice and SMS agents.
The result is an average 47% reduction in administrative overhead across the workflows that matter most, based on Clustox implementation data across DME clients on Brightree and NikoHealth.
This article maps those workflows, explains how the automation works at a technical and operational level, provides an honest account of what it does not handle yet, and gives you a structured checklist for evaluating whether your operation is ready to make the same move.
What This Article Covers
- Why administrative overhead is the primary margin threat for DME operators in 2026
- The six workflows where healthcare automation delivers the highest return in DME
- How Agentic AI workflows operate on top of Brightree and NikoHealth technically and practically
- A phased implementation roadmap from audit to full deployment
- Real benchmark numbers from DME operations running AI-automated workflows
- What automation does not handle yet and where human oversight remains essential
- A buyer’s checklist for evaluating healthcare automation vendors
Why Administrative Overhead Is the Primary Margin Threat for DME Operators
CMS Competitive Bidding Round 2024 reduced reimbursement rates for high-volume HCPCS categories by an average of 23%, according to AAHomecare’s 2024 Competitive Bidding analysis. At the same time, CMS expanded prior authorization requirements to five additional product categories under the Medicare Prior Authorization Program.
Payer audit activity through TPE, RAC, ZPIC, and UPIC programs has increased, adding documentation burden to every order. Staffing costs have not come down.
The math is unforgiving. Lower reimbursement per order plus higher administrative cost per order equals a margin problem that cannot be solved by working harder. The only operational lever available is the cost per order, and the only way to reduce that cost at scale, without reducing headcount or quality, is automation.
Table of Contents
Key Benchmarks
Prior auth processing time: 6–9 days (manual baseline), per HFMA 2024 Revenue Cycle Benchmarking Report.
DME claim write-off rate: 6–12% of submitted claims, per OIG 2023 DME billing compliance report.
Administrative cost per claim: $25–$50 for manually processed DME orders, per HFMA.
Staff capacity constraint: manual billing teams typically cap at 80–120 complex orders per month.
Healthcare workflow automation in DME addresses the cost-per-order problem directly. By removing manual touchpoints from prior auth, eligibility, intake, and denial management, the same billing team can process two to three times the order volume without adding headcount and without reducing documentation quality. That is the margin lever that AI-first operators are pulling.
The Six High-Return Workflows for DME Automation
Not every DME workflow benefits equally from automation. The six workflows below consistently deliver the highest return across DME operations of different sizes and payer mixes.
They are ordered by typical implementation priority: start with prior authorization and eligibility, then add denial management, intake, resupply, and recertification as the foundation stabilizes.
1. Prior Authorization Submission and Follow-Up
Prior authorization is the highest-volume manual workflow in most DME billing departments. Every complex order of CPAP devices under HCPCS E0601, oxygen concentrators under E1390, and power wheelchairs under K0800–K0899 requires documentation gathering, payer portal submission, status monitoring, and escalation for stalled requests. Each of these steps is currently done by a human, for every order, every time.
An Agentic AI prior auth workflow built on LangGraph handles the full cycle: it pulls the order and Letter of Medical Necessity (LMN) from Brightree or NikoHealth, verifies documentation completeness against CMS coverage criteria and payer-specific PA requirements, submits via the payer portal or fax API, monitors status automatically, and routes only genuine exceptions peer-to-peer escalations, non-standard denials, and missing clinical information to a human reviewer.
The result is prior auth turnaround time dropping from 6 to 9 days to under 48 hours for standard categories. The billing team shifts from processing every PA to reviewing the 10 to 15% that require human judgment.
2. Eligibility and Benefits Verification
A single eligibility check at intake is not enough. Patients in Medicare Advantage plans can have benefit changes mid-year. Coordination-of-benefits situations shift primary payer responsibility. Recurring supply orders for CPAP or oxygen can hit benefit limits without the billing team knowing until the claim drops and comes back denied.
AI eligibility verification agents run real-time 270/271 checks at three defined points: at order intake, at prior authorization submission, and at claim drop. They flag benefit-limit proximity alerting when a patient is within 15% of an annual HCPCS benefit cap and route coordination-of-benefits exceptions to a human before the claim goes out wrong. Multi-point verification reduces eligibility-driven soft denials by 15 to 22%, per Clustox implementation data across Brightree and NikoHealth clients.
3. Denial Management and Appeals
Soft denials are recoverable revenue that most DME billing teams do not have time to pursue systematically. The average provider writes off 6 to 12% of submitted claims, according to OIG’s 2023 DME billing compliance report. Most of that write-off is soft denials: documentation gaps, coding mismatches, authorization discrepancies, and timely filing issues, all correctable on appeal if caught quickly and worked efficiently.
Agentic AI denial management classifies every incoming denial by root cause, drafts the appropriate appeal letter with the correct supporting documentation, LMN, payer-specific clinical criteria, and HCPCS modifier corrections, and submits the appeal within the payer’s window automatically.
It also feeds denial patterns upstream: if a specific payer consistently denies E1390 claims without a specific ICD-10 code on the supporting documentation, the prior auth workflow is updated to include it on future submissions. DMEs implementing this workflow recover 18 to 27% of previously written-off soft denials within 90 days.
4. Patient Intake and Qualification
New patient intake in DME is administratively heavy. Collecting insurance information, verifying coverage, confirming referring physician orders, checking HCPCS qualification criteria, and creating the order in Brightree or NikoHealth can take a trained billing coordinator 45 to 60 minutes per patient before a single claim has been submitted.
AI patient intake agents handle the structured portions of this workflow automatically: they pull referral orders, verify insurance via real-time eligibility checks, confirm qualification criteria against CMS coverage requirements for the ordered product category, and pre-populate the order record in the practice management platform. The billing coordinator reviews a completed intake record rather than building one from scratch. Staff time per intake drops from 45 to 60 minutes to 8 to 12 minutes for standard cases.
5. CPAP Re-Supply Outreach
CPAP re-supply is one of the highest-margin, most predictable revenue streams in DME and it leaks constantly through patient non-response. Patients who do not receive a re-supply outreach call, or who do not respond to paper mailers, do not reorder. For operations running hundreds of active CPAP patients, that non-response compounds month over month into meaningful lost revenue.
AI voice agents and SMS agents contact patients on their preferred channel at the appropriate re-supply interval, typically every 90 days for masks and supplies and every 6 months for CPAP devices, to confirm re-supply needs, capture refusals or deferrals, and push confirmed orders directly back into Brightree or NikoHealth for fulfillment. No billing coordinator time is required for routine outreach.
Providers running AI re-supply outreach report 30 to 40% improvement in monthly re-supply order capture compared to phone-only outreach, according to Clustox implementation data.
6. Oxygen Recertification Workflow Automation
Oxygen recertification is one of the most compliance-sensitive workflows in DME. CMS requires recertification of oxygen orders at specific intervals, typically at 90 days and annually, with updated clinical documentation from the referring physician. Missing a recertification window results in claim denials and potential audit exposure. Tracking and managing these deadlines manually across hundreds of active oxygen patients is a significant administrative burden.
Automated recertification workflows monitor recertification dates for every active oxygen patient, send alerts to the ordering physician’s office 30 and 14 days before the deadline, collect updated documentation, and flag any patients whose recertification is at risk of lapsing. The billing team is notified only for exceptions, patients whose physicians have not responded and where manual escalation is required. Near-zero missed recertifications is achievable with a properly configured workflow.
How Healthcare Workflow Automation Works in DME: The Technical Architecture
Understanding the architecture matters if you are evaluating vendors or making a build-vs-buy decision. Healthcare workflow automation in DME is not a single product. It is a layered system with four components working together.
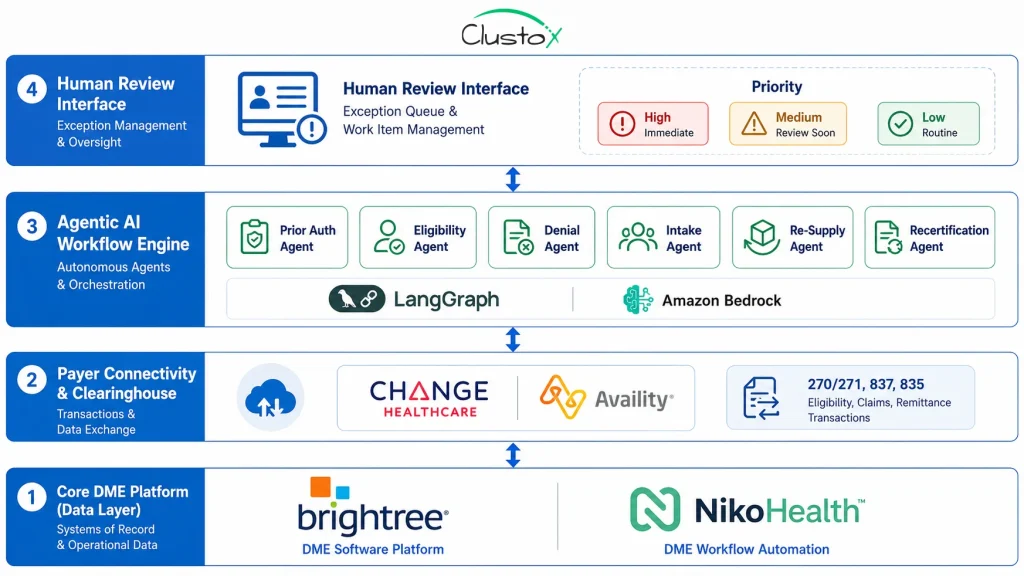
Component 1: The Core DME Platform (Data Layer)
Brightree or NikoHealth is the foundation. All patient records, orders, claims, and payer interactions live here. The AI layer reads from and writes back to this system via API, pulling order data, pushing status updates, creating intake records, and logging every automated action for audit trail compliance.
API access quality is the single biggest determinant of implementation cost and timeline. Brightree provides API access through its integration framework.
NikoHealth provides modern REST API access that is faster and less expensive to integrate. Older platforms such as TIMS have limited API surfaces that significantly increase integration complexity.
Component 2: The Payer Connectivity Layer
EDI transactions, 270/271 eligibility queries, 837 claim submissions, and 835 remittance files flow between the DME platform and payers through a clearinghouse such as Change Healthcare or Availity, or through direct payer connections for high-volume relationships. The AI layer uses this connectivity to run real-time eligibility checks and to submit and monitor prior authorization requests.
Component 3: The Agentic AI Workflow Engine
This is where the automation actually runs. Agentic AI workflows built on orchestration frameworks such as LangGraph and deployed on HIPAA-compliant infrastructure such as AWS Bedrock are goal-directed systems that can complete multi-step tasks without human input at each step.
They are not chatbots, and they are not simple rule engines. They navigate real payer portals, handle non-standard responses, make conditional decisions based on payer-specific policy, and escalate to humans only when genuine exceptions occur.
Each workflow is a defined agent with a specific goal: the prior auth agent’s goal is to get a prior authorization approved. The eligibility agent’s goal is to confirm accurate coverage before the claim drops. The denial agent’s goal is to recover denied revenue within the payer’s appeal window. These agents run continuously across all active orders, not just the ones a billing coordinator has time to reach.
Component 4: The Human Review Interface
Automation does not eliminate the billing team. It changes what the billing team does. Instead of processing every order from scratch, billing coordinators review exception queues: prior auth requests that require peer-to-peer escalation, eligibility situations that require manual investigation, and appeal letters that require a human signature before submission. The interface surfaces exceptions clearly, with all relevant documentation assembled by the AI agent, so the coordinator can act in minutes rather than hours.
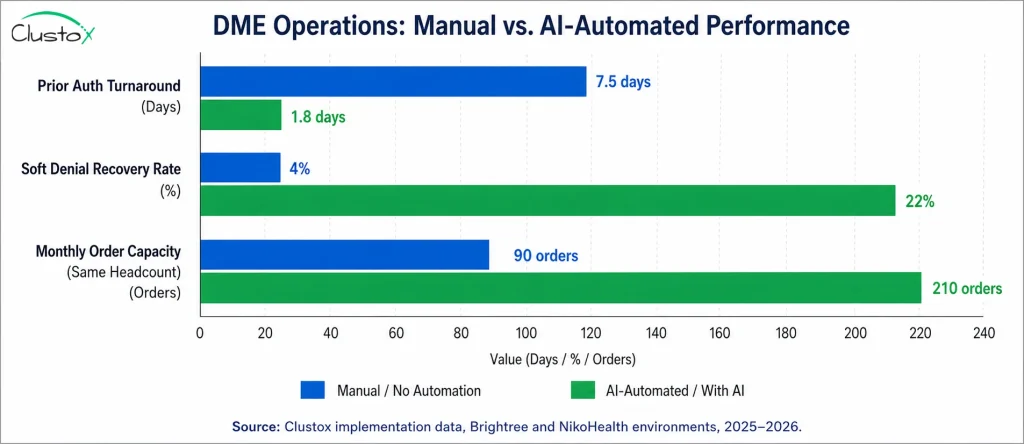
Real Numbers: What DME Operators Are Seeing
The following benchmarks reflect Clustox implementations across DME clients on Brightree and NikoHealth. These are operational results across the six automation workflows described above. Results vary by payer mix, order volume, and existing workflow maturity.
Numbers sourced from Clustox client data, HFMA 2024 Revenue Cycle Benchmarking, AAHomecare 2024 analysis, and OIG 2023 DME billing compliance data.
| Workflow | Manual Baseline | With AI Automation | Improvement |
|---|---|---|---|
| Prior Authorization | 6–9 days per order | Under 48 hours | 75–80% faster |
| Eligibility Verification | 15–25 min per check, manual | Real-time (seconds) | Errors down 15–22% |
| Denial Management | 6–12% write-off rate | 18–27% denials recovered | Revenue recovery |
| Patient Intake & Qualification | 45–60 min staff time per patient | 8–12 min (AI-assisted) | 80% time reduction |
| CPAP Re-Supply Outreach | Phone-only, 30–40% reach | Voice + SMS, 65–75% reach | 30–40% more orders |
| Oxygen Recertification | Manual tracking, high miss rate | Automated alerts + doc collection | Near-zero missed certs |
| Overall Admin Overhead | Baseline | 47% reduction | Same headcount, 2–3x volume |
Implementation Roadmap: From Audit to Full Deployment
DME operations that try to automate everything at once typically do not automate anything well. The implementations that succeed follow a phased approach: start with the highest-volume, highest-friction workflow, prove the model, then expand.
The table below shows a typical six-phase roadmap from initial AI readiness audit through full multi-workflow deployment.
| Phase | Activities | Timeline | Prerequisites |
|---|---|---|---|
| Audit | Map current workflows; identify top 3 admin bottlenecks; confirm API access on Brightree or NikoHealth | Days 1–2 | Platform access, billing team availability |
| Design | Define agent workflows for priority use cases; map payer-specific PA rules; design eligibility check cadence | Weeks 1–2 | Workflow maps, payer policy library |
| Build | Deploy prior auth agent; integrate eligibility verification; configure LMN documentation checks | Weeks 3–6 | API credentials, HIPAA BAA with infrastructure provider (AWS Bedrock) |
| Test | Run parallel with manual workflow; validate accuracy on 200+ orders; tune exception handling | Weeks 7–8 | Test dataset, billing team review time |
| Go Live | Cut over to AI-first workflow; monitor daily for first 30 days; document exception patterns | Week 9+ | Training for billing team on exception review |
| Expand | Add denial management agent; CPAP re-supply voice/SMS; oxygen recertification alerts | Months 4–6 | Stable prior auth and eligibility baseline |
Most operations reach a positive ROI position within the first billing cycle after Phase 3 goes live, typically 30 to 60 days after deployment, through recovered soft denials and prior authorization acceleration alone. The full 47% admin reduction is typically achieved after Phase 6, when all six workflows are running in production.
Prerequisites: What You Need Before You Start
The single most common reason DME AI implementations take longer than planned is insufficient preparation. Here is what needs to be in place before the build phase begins.
1. Platform API Access
Confirm that your practice management platform, Brightree or NikoHealth, provides API access at the level required for the workflows you want to automate. For Brightree, this means confirming integration partner credentials and understanding the API rate limits. For NikoHealth, REST API access is standard. For TIMS or other legacy platforms, conduct a technical feasibility review before committing to an AI implementation timeline.
2. HIPAA BAA with Infrastructure Provider
All AI processing of Protected Health Information (PHI) must occur under a signed HIPAA Business Associate Agreement with the infrastructure provider. AWS Bedrock, Azure OpenAI Service, and Google Cloud Vertex AI are the three primary BAA-eligible options for DME Agentic AI workflows. This agreement must be in place before any PHI is passed to the AI layer. HHS guidance on HIPAA BAA requirements is available at HHS.gov.
3. Payer Policy Library
The prior auth agent needs to know the PA requirements for each payer and product category combination your operation bills. This means maintaining an up-to-date payer policy library CMS coverage criteria for each relevant HCPCS code, Medicare Advantage plan-specific PA rules, and Medicaid state program requirements where applicable. Without this library, the agent cannot accurately assess documentation completeness before submission.
4. Clean Data in Your Core Platform
AI automation is only as accurate as the data it reads from. Patient records with incomplete insurance information, orders with missing referring physician data, and claim records with unresolved coding errors will create exception rates that undermine the efficiency gains. A data quality review of your Brightree or NikoHealth instance before implementation is not optional it is what the audit phase in the roadmap is designed to catch.
5. Billing Team Preparation
The billing team’s role changes significantly after automation goes live. They move from order processors to exception reviewers. This is a meaningful shift in how they spend their day, and it requires clear communication, training on the exception review interface, and a defined escalation protocol for edge cases.
Operations that do not invest in this preparation typically see higher exception rates in the first 30 days as the team works to understand what the AI is routing to them and why.
What Doesn’t Work Yet: Current Limits of DME Workflow Automation
The results above are real. So are the limits. Treating automation as a complete solution without understanding its boundaries leads to poorly designed exception handling and, eventually, to claim errors that cost more to fix than the automation saved.
1. Non-Standard Payer Portal Interfaces
AI agents work most cleanly on payer portals with consistent, well-documented interfaces. Some regional Medicare Advantage plans and Medicaid managed care organizations use non-standard portals that do not expose predictable fields or navigation paths.
For these payers, the agent requires a manual fallback path until the portal interface is mapped and the agent is trained on it. Expect 10 to 20% of your payer mix to require manual fallback at initial deployment, declining over time as the agent learns.
2. LMN Quality from Referring Physicians
An AI documentation check confirms whether a Letter of Medical Necessity is present and whether it contains the required elements for the relevant HCPCS category and payer. It cannot fix a clinically inadequate LMN.
If the referring physician’s documentation does not meet coverage criteria, the agent will flag it as incomplete and route it to a human, but the underlying problem is a referral relationship issue that technology cannot solve. Practices with weak referring physician relationships will see higher documentation-driven PA denial rates regardless of automation quality.
3. Complex Rehab Technology and Custom Equipment
For CRT categories custom power wheelchairs (K0800–K0899), complex seating systems, and custom orthotics, documentation requirements are highly individualized and payer-specific. Clinical justification standards vary significantly by plan.
Automation assists with documentation completeness checks and submission logistics, but the clinical review and coverage determination for these categories still requires a trained specialist. Do not attempt to fully automate CRT prior authorization without a human clinical reviewer in the loop.
4. TPE, RAC, ZPIC, and UPIC Audit Response
AI can assemble documentation packages for Medicare audit responses organizing claim records, pulling supporting clinical documentation, and formatting the response according to audit contractor requirements. However, the substantive review of audit findings and the decision about how to respond requires human expertise and, in some cases, legal counsel. Automating the assembly work is appropriate. Automating the response decision is not. The OIG is clear that providers bear responsibility for the accuracy and completeness of their audit responses.
5. Multi-System Legacy Environments
Operations running TIMS alongside a secondary billing system and manual spreadsheet workflows have significantly higher integration complexity than those on a single modern platform.
The AI layer requires clean, consistent data access, which is difficult to achieve when data lives in multiple systems with inconsistent record structures. If you are in this position, the most cost-effective path is often platform consolidation before AI implementation, not simultaneously with it.
Buyer’s Checklist: Evaluating Healthcare Workflow Automation Vendors
If you are evaluating vendors or implementation partners for DME workflow automation, these are the questions that separate a solid implementation from one you will spend the next 18 months fixing.
- API integration depth. Ask specifically: which fields, objects, and actions are available via API in your current platform? Can the vendor demonstrate a live integration with Brightree or NikoHealth, not a generic demo environment?
- Prior auth completion rate. What percentage of prior authorization submissions are completed end to end by the AI agent without human intervention? For well-configured workflows on major payers, this should exceed 85%. If the vendor cannot give you a number, they do not know.
- Payer coverage. How many of your top 10 payers are fully supported? For which payers does the agent require a manual fallback? Get this in writing.
- HIPAA infrastructure. Which infrastructure provider is used for AI processing? Is a BAA in place? Can they provide documentation? This is a compliance requirement, not a checkbox.
- Exception rate benchmarks. What is the typical exception rate at go-live and at 90 days post-deployment? A vendor who cannot quantify their exception rates has not measured their own performance.
- Implementation timeline and support. What is the realistic go-live timeline from signed contract, including the audit and design phases? Who owns the data migration? What is the escalation path if integration fails during testing?
- ROI measurement methodology. How will improvement be measured? What baseline data do they need, and when will they provide a post-implementation report? Vendors who do not measure ROI do not expect to deliver it.
- Audit trail and compliance logging. Does every automated action every prior auth submission, every eligibility check, and every denial appeal produce a timestamped, attributable audit log? This is essential for TPE and RAC audit defense.
Frequently Asked Questions
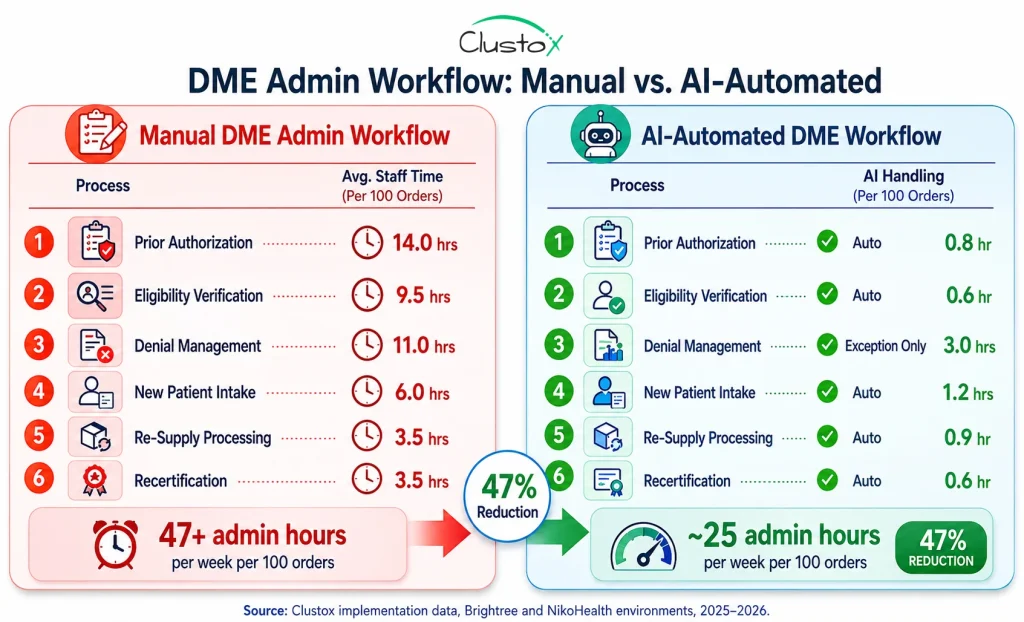
How does the 47% admin reduction figure translate to actual hours saved?
For a DME operation processing 100 complex orders per month, manual administrative workflows typically consume 47 or more staff hours per week across prior auth, eligibility, denial management, and intake. AI-automated workflows reduce that to approximately 25 hours per week for the same volume, with the remaining hours focused on exception review. The 47% figure reflects the net reduction across all six automation workflows at full deployment, based on Clustox implementation data.
Does healthcare workflow automation work with both Brightree and NikoHealth?
Yes. Brightree and NikoHealth are the two platforms with sufficient API access to support full Agentic AI integration. Brightree integrations typically take longer and cost more due to its older API architecture but are well-established and reliable. NikoHealth's modern REST API makes integration faster and less expensive. Legacy platforms such as TIMS have limited API surfaces that make full automation significantly more complex.
Is Agentic AI for DME workflows HIPAA compliant?
It can be, but compliance requires deliberate architecture. All AI processing of Protected Health Information must occur under a signed HIPAA Business Associate Agreement with the infrastructure provider. AWS Bedrock, Azure OpenAI Service, and GCP Vertex AI offer BAA-eligible environments. HIPAA compliance is an architecture requirement; it must be built in, not added on after deployment. HHS has published guidance on BAA requirements at HHS.gov.
Which workflow should a DME operation automate first?
Prior authorization is the right starting point for most operations. It is the highest-volume manual workflow, the one where time-to-completion most directly affects revenue, and the one where AI performance is most measurable. Once prior authorization automation is stable, eligibility verification is the natural second step; it prevents the downstream claim errors that denial management then has to clean up. Denial management, intake, resupply, and recertification follow in that order for most operations.
How long does a full DME workflow automation implementation take?
A phased implementation covering prior authorization and eligibility verification typically reaches go-live in 8 to 12 weeks from the signed contract, assuming API access is confirmed and the audit phase is completed efficiently. Full multi-workflow deployment, adding denial management, intake, resupply, and recertification, typically takes 4 to 6 months. Operations with data quality issues or legacy platform complexity should add 4 to 8 weeks to these timelines.
What happens to billing staff when workflows are automated?
Billing staff shift from processing every order to reviewing exceptions. Instead of building prior auth submissions from scratch, they review flagged cases complex peer-to-peer escalations, documentation gaps that the AI could not resolve, non-standard payer responses. This is a meaningful change in the day-to-day role, and it requires clear communication and training. Operations that handle this transition well typically see improved job satisfaction, because staff spend more time on judgment-based work and less on repetitive data entry.
What is the ROI timeline for DME healthcare workflow automation?
Most operations see measurable ROI within the first billing cycle after the prior authorization and eligibility workflows go live typically 30 to 60 days. Denial recovery ROI appears within 90 days of the denial management workflow deployment. Re-supply revenue uplift appears in the first re-supply cycle post-deployment. Full ROI across all six workflows is typically realized within 6 months of complete deployment.
Can automation handle Medicare audit responses for TPE or RAC audits?
Partially. AI automation can assemble the documentation package for a TPE or RAC audit response, pulling the relevant claim records, supporting clinical documentation, and formatting the response package according to audit contractor requirements. However, the substantive review of audit findings and the decision about how to respond requires human expertise and, in some cases, qualified healthcare counsel. Do not automate the response decision, only the documentation assembly.
How do I know if my DME operation is ready for workflow automation?
The key variables are API access quality on your current platform, data quality in your patient and claim records, billing team readiness to shift to an exception-review model, and leadership clarity on which workflow to automate first. A 48-hour AI Readiness Audit maps all of these variables and produces a prioritized workflow plan with a fixed-cost ROI model before you commit to any implementation spend.
Conclusion
The 47% reduction in administrative overhead is not a projection. It is what happens when DME operations systematically remove the manual touchpoints from the six workflows that consume the most billing team time: prior authorization, eligibility verification, denial management, patient intake, CPAP re-supply outreach, and oxygen recertification. Each workflow has a defined automation path. Each one delivers a measurable result within the first billing cycle or two after deployment.
The technology to do this is available and production-tested on Brightree and NikoHealth. The architecture for doing it in a HIPAA-compliant environment is well-established. The implementation path is phased and predictable. What varies is the readiness of the operation, the quality of data in the core platform, the accessibility of the API, and the clarity of leadership on where to start.
The operators who are gaining the most ground right now are not waiting for a perfect moment. They are starting with prior authorization, the highest-friction, highest-volume workflow, proving the model in the first 90 days, and expanding from there.
By the time their competitors are evaluating whether to begin, they are already processing three times the volume with the same team.
If you want to understand what that looks like for your specific operation, your payer mix, your platform, and your current workflow friction, that is exactly what the AI Readiness Audit maps out in 48 hours, at a fixed price.