
A denied claim usually starts as a small mistake that no one noticed in time. A missing modifier. An invalid diagnosis-to-procedure pairing. A prior authorization number that never made it into the claim. A rendering provider NPI mismatch. By the time the denial appears on the 835 ERA, the payment delay, rework, and staff cost have already happened.
The financial impact is larger than most healthcare operators realize. According to the HFMA Revenue Cycle Benchmarking Report, the average denied claim costs providers approximately 118 dollars when rework, appeals, and write-offs are included.
For DME providers, first-pass denial rates typically range between 15% and 18%, significantly higher than the broader healthcare industry average. The majority of these denials are not complex payer disputes; they are preventable submission errors that should have been caught before the claim ever left the system.
AI-powered pre-submission review changes where denial prevention happens. Instead of identifying errors weeks later during remittance processing, AI reviews the claim before submission, flags missing or inconsistent data in real time, and routes the claim into a correction workflow before it reaches the payer.
This guide explains how AI-driven claims review works, which denial categories it can reliably prevent, where human review is still necessary, and what implementation looks like for healthcare and DME organizations using Brightree, NikoHealth, or clearinghouse-connected billing workflows.
What Does This Guide Cover?
- The most common pre-submission claims errors that AI can detect and prevent
- How AI pre-submission review works inside a healthcare claims workflow
- Where AI fits alongside traditional claim scrubbing and clearinghouse edits
- Error categories AI handles well versus those that still require human review
- Real denial reduction benchmarks from DME and healthcare operators
- Implementation requirements and integration with Brightree and NikoHealth
- Limits, risks, and what to watch for before deploying AI in your claims workflow
- Eight frequently asked questions from billing directors and revenue cycle managers
What Are the Most Common Pre-Submission Claims Errors in Healthcare?
Healthcare claim errors fall into seven categories. Understanding which category each error belongs to matters because the AI detection approach is different for each one. CMS publishes Annual Medicare Fee-for-Service Improper Payment Data that breaks down improper payment causes by type. The 2023 report attributes more than 31 billion dollars in Medicare improper payments to documentation errors alone, with billing and coding errors accounting for a further 6.8 billion dollars.
1. Coding Errors: Wrong ICD-10, HCPCS, or CPT Code
Coding errors are the most common claim error category in DME billing. They include using an ICD-10 diagnosis code that does not support the equipment ordered, assigning the wrong HCPCS Level II code for the specific equipment configuration, and selecting a CPT code that does not match the procedure or service documented. For DME specifically, HCPCS Level II code assignment is complicated by the specificity requirements for power mobility devices, oxygen equipment, and CPAP supplies, where a single code change (E0601 versus E0470, for example) changes the reimbursement rate and coverage criteria significantly. Reference: CMS HCPCS code set lookup.
2. Modifier Errors: Missing, Wrong, or Conflicting Modifiers
Modifier errors cause approximately 16 percent of DME claim denials, per HFMA DME benchmark cohort data. The highest-risk modifiers in DME billing are KX (indicating that documentation meets the LCD coverage criteria), GA (indicating a signed ABN is on file), GY (item is statutorily excluded), and GZ (item expected to be denied as not medically necessary). Applying KX without supporting documentation is not just a denial risk; it is an audit risk. Missing the modifier entirely is an automatic denial for many payers. For rental equipment categories, the NU (new equipment), RR (rental), and UE (used equipment) modifier requirements must also be applied correctly for each rental month. Reference: CMS modifier guidance.
Table of Contents
3. Documentation Gaps: Missing or Non-Compliant Supporting Documents
Documentation errors are the largest single category of DME improper payments, accounting for approximately 28 percent of denials per HFMA benchmark data and more than 31 billion dollars annually in Medicare improper payments per CMS 2023 data.
Documentation errors include missing Detailed Written Orders (DWO), Letters of Medical Necessity (LMN) that do not cover the prescribed equipment, unsigned or expired DWOs, missing face-to-face encounter notes, and proof of delivery (POD) gaps. AI can verify whether required documents are present in the order record, but cannot assess whether the clinical content of those documents meets the payer’s medical necessity criteria.
4. Eligibility Errors: Inactive Coverage or Wrong Plan
Eligibility errors cause approximately 22 percent of DME denials and contribute to more than 1.2 billion dollars in annual DME improper payments, per CMS 2023 Medicare improper payment data.
These include billing a payer whose coverage lapsed before the date of service, billing Medicare Part B for a patient enrolled in a Medicare Advantage plan, using an incorrect member ID or group number, and missing coordination of benefits (COB) when a patient has multiple payers.
5. Prior Authorization Errors: Missing, Expired, or Wrong Code
A missing prior authorization is an automatic denial with no appeal path for equipment categories covered under the CMS Prior Authorization program for DME. PA errors include submitting a claim without any PA on file, using an expired PA approval, and submitting a claim under a HCPCS code that is different from the code the PA was approved for. These account for approximately 19 percent of DME denials per HFMA benchmark data.
6. Timely Filing Violations: Claims Submitted Outside the Filing Window
Timely filing violations are entirely preventable with automated claim submission monitoring. Medicare Part B DME has a 12-month timely filing limit from the date of service. Most Medicare Advantage plans have shorter filing windows, often 90 to 180 days. Timely filing denials account for approximately 9 percent of DME denials and are not appealable once the window closes; the revenue is gone. Reference: CMS timely filing guidance via the Medicare Learning Network.
7. Duplicate Claim Errors: Resubmission Without Correct Claim Frequency Code
Duplicate claim denials occur when a claim is submitted more than once for the same service date and patient without the correct claim frequency code to indicate that it is a corrected or replacement claim. This is most common when billing staff resubmits claims after a denial without updating the frequency code from 1 (original) to 7 (replacement) or 8 (void). The result is a duplicate denial on top of the original denial, doubling the rework cost.
How Does AI Catch Healthcare Claims Errors Before Submission?
AI pre-submission review operates as a layer that sits between claim creation in the core billing platform and electronic submission to the payer via the clearinghouse. It is not a replacement for traditional claim scrubbing.
It runs in addition to the rule-based scrubber and catches a different and more complex category of errors that rule-based systems consistently miss.
The process runs in 4 stages:
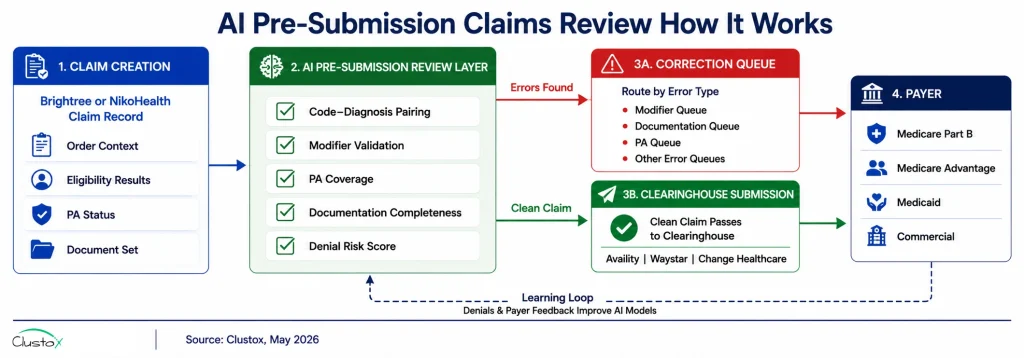
Stage 1 Claim Ingestion and Context Assembly
When a claim is created in Brightree, NikoHealth, or the clearinghouse integration (Availity, Waystar, or Change Healthcare), the AI agent ingests the claim data alongside its full context: the order record, the patient eligibility results, the PA status, the document set on file (DWO, LMN, POD), the payer’s Local Coverage Determination (LCD) for the HCPCS code billed, and the historical denial pattern for this payer and code combination.
Rule-based scrubbers check the claim in isolation. The AI review checks the claim against everything that should support it.
Stage 2 Multi-Layer Error Analysis
The AI agent runs 5 concurrent checks:
- Code-diagnosis pairing validation: The ICD-10 diagnosis code is checked against the HCPCS code to confirm the diagnosis supports the equipment under the payer’s current LCD. Code pairs that have a documented denial history for this payer are flagged even if they are technically valid under CMS national policy.
- Modifier completeness and conflict check: Required modifiers are confirmed for the specific payer, equipment category, and rental month. Conflicting modifier combinations (for example, KX and GY cannot appear on the same claim) are flagged automatically.
- PA coverage confirmation: The PA on file is checked against the claim date, the specific HCPCS code billed, and the approved equipment category. A PA approved for E0601 does not cover a claim billed under E0470.
- Documentation completeness check: Required document types (DWO, LMN, POD) are confirmed as present in the order record and checked for basic validity signals: DWO signature present, DWO date within 12 months, and LMN covers the prescribed equipment category.
- Denial risk scoring: The claim is scored against the historical denial pattern for this payer, code, and documentation combination. Claims that share characteristics with previously denied claims are flagged for pre-submission human review rather than being submitted and generating a predictable denial.
Stage 3 Error Routing and Correction Queue
Claims with identified errors or a denial risk score above the configured threshold route to a correction queue specific to the error type, a modifier error queue, or a documentation gap queue. Each queue presents the specific error alongside the claim detail and the recommended correction action. Staff correct and resubmit from the queue rather than reprocess the claim from scratch.
Claims that pass all checks are submitted to the payer via clearinghouse without any manual intervention. The clean claim rate for claims that pass AI pre-submission review is consistently above 92 percent in Clustox client operations (2024 to 2025, anonymized composite data).
Stage 4 Learning Loop and Denial Pattern Update
When a denial is received on a claim that passed AI pre-submission review, the denial reason is fed back into the AI model to update its denial risk scoring for that payer, code, and documentation combination. This learning loop means the system becomes more accurate over time as it accumulates payer-specific denial pattern data. A static rule-based scrubber does not learn from denials. The AI layer does.
How Does AI Pre-Submission Review Differ From Traditional Claim Scrubbing?
Traditional claim scrubbing and AI pre-submission review are complementary tools that operate at different levels of the claims workflow. Understanding the difference prevents the common mistake of treating them as alternatives.
What Does a Traditional Claim Scrubber Do?
A traditional claim scrubber is a rules-based system that checks a claim against a defined set of edit rules before submission. Those rules check for formatting errors (valid NPI format, required field completion, valid date ranges), basic code validity (CPT and ICD-10 codes exist and are currently active), and known invalid combinations (procedure code not consistent with the listed diagnosis based on CMS national edits). Rule-based scrubbers are fast, reliable, and well-suited to catching formatting and structural errors. They do not learn from denial patterns, cannot assess context, and cannot predict payer-specific denial risk.
What Does AI Pre-Submission Review Add?
AI pre-submission review adds contextual analysis that rule-based scrubbers cannot perform. Specifically, it checks the claim against the patient’s eligibility results, the PA on file, the document set in the order record, the payer’s LCD, and the historical denial pattern for this payer-code combination.
It scores denial risk based on pattern matching across thousands of prior claims rather than matching against a fixed rule set. And it routes errors to specific correction queues based on error type rather than presenting a generic failed edit list.
The practical result is that AI review catches the errors that scrubbers consistently miss: the KX modifier applied when the documentation does not support it, the PA that is on file but covers the wrong HCPCS code, the LMN that is present in the record but expired, and the ICD-10 diagnosis that is technically valid but has a high historical denial rate for this specific payer.
These are judgment-level errors, not formatting errors, and they are the primary driver of the 15 to 18 percent DME denial rate.
Where Does the Clearinghouse Edit Fit?
Clearinghouse edits (the 277CA acknowledgment from Availity, Waystar, or Change Healthcare) are a third layer that catches formatting and routing errors after the claim leaves the billing platform but before it reaches the payer.
A claim that passes AI pre-submission review and the claim scrubber should rarely fail a clearinghouse edit. When clearinghouse rejections do occur on AI-reviewed claims, they typically indicate a payer enrollment or routing configuration issue rather than a claim content error.
What Results are Healthcare and DME Operators Seeing With AI Claims Review?
The benchmarks below combine published industry data with operator-reported outcomes from DME and healthcare billing operations that implemented AI pre-submission review during 2024 and 2025.
Individual results vary by payer mix, error profile, and implementation quality.
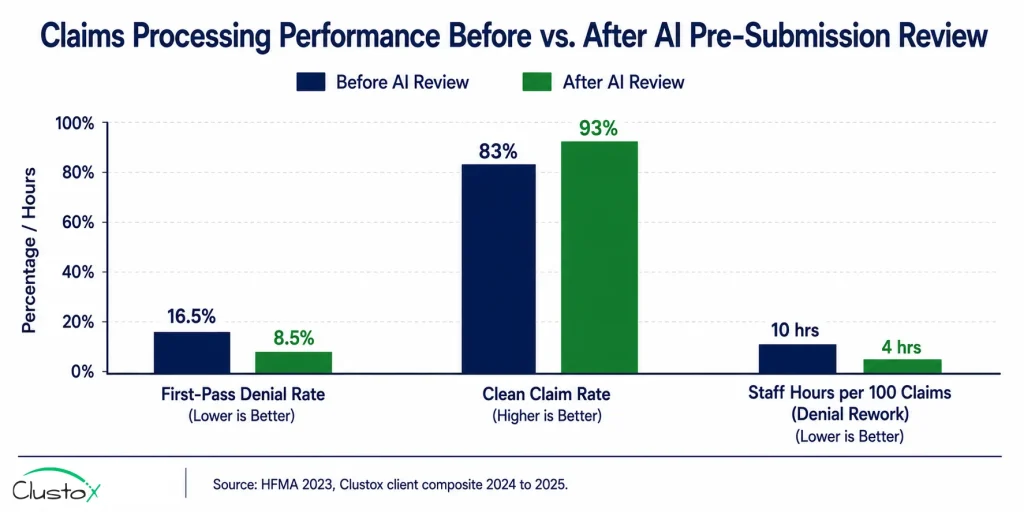
1. Denial Rate Reduction
First-pass claim denial rates for DME operations using AI pre-submission review consistently reach 7 to 10 percent, compared to the 15 to 18 percent industry baseline, per HFMA DME benchmark cohort data. The improvement is most pronounced in modifier error denials (which typically drop by 70 to 80 percent) and eligibility error denials (which drop by 60 to 75 percent), since both categories are highly detectable at the pre-submission stage.
2. Cost Per Claim Reduction
At 118 dollars per denied claim in rework cost, reducing the denial rate from 17 percent to 9 percent on a 400-claim-per-month operation saves approximately 38 denied claims per month, generating 4,484 dollars in monthly rework cost reduction before accounting for recovered claim revenue. HFMA reports the average cost to collect per claim falls from 8 to 14 dollars to 5 to 9 dollars for operations that reduce denial rework cycles through pre-submission review.
3. Clean Claim Rate Improvement
Clean claim rates for claims that pass AI pre-submission review sit above 92 percent in Clustox client operations (2024 to 2025, anonymized composite data). Operations without AI review typically report clean claim rates of 82 to 85 percent. The 7 to 10 percentage point improvement in clean claim rate compounds across claim volume; each percentage point improvement represents approximately 4 additional clean claims per 400 monthly submissions, at an average reimbursement of 350 dollars per DME claim.
4. Staff Time on Denial Rework
Staff hours spent on denial rework per 100 claims drops from 8 to 12 hours to 3 to 5 hours for operations using AI pre-submission review, per Clustox client composite data. The reduction comes primarily from fewer denials entering the rework queue, not from AI handling the rework itself.
The rework that does occur is better organized, routed to specific queues by error type rather than presented as an undifferentiated denial list, which improves resolution speed per denial even when volume reduction is modest.
How Do You Implement AI Pre-Submission Claims Review?
AI pre-submission review is not a standalone product; it is a layer that connects to the existing claims workflow via API. Implementation requires a platform with an open API, clearinghouse enrollment, and a defined error routing workflow before the AI layer can add value.
What Prerequisites Are Required Before Implementation?
- Core platform API access: The AI review layer reads claim data, order records, eligibility results, and document sets from Brightree or NikoHealth via API. If the platform has a limited or undocumented API, the AI layer cannot access the context it needs to perform contextual error analysis. Confirm API access is enabled and documented before any implementation planning begins.
- Clearinghouse enrollment: Active enrollment with at least one of Availity, Waystar, or Change Healthcare is required for claim submission. The AI layer connects between the billing platform and the clearinghouse, so clearinghouse enrollment must be current and functioning before the AI layer is added.
- 270/271 EDI eligibility integration: AI denial risk scoring is significantly more accurate when the claim is evaluated alongside real-time eligibility results rather than eligibility data that was collected days earlier and may have changed. Real-time eligibility integration is a prerequisite for the eligibility error detection component of AI review.
- HIPAA-compliant infrastructure: The AI layer processes PHI when it reads claim and order records. A signed Business Associate Agreement (BAA) with the AI platform vendor, SOC 2 Type II certification, and US-only data residency are required before any PHI touches the AI system.
- Defined correction queue workflow: AI pre-submission review only adds value if the errors it identifies are corrected before submission. A defined correction queue with assigned staff, correction SLAs, and escalation paths must be in place before the AI layer goes live. Routing errors into a queue that nobody monitors is worse than not routing at all, because it creates the impression that the AI is working when claims are actually sitting uncorrected.
What Does the Implementation Timeline Look Like?
- Week 1 to 2 (Discovery): Map the current claims workflow, identify error categories driving the highest denial volume, confirm API access and clearinghouse connectivity, and review the payer mix to prioritize payer-specific rule configuration.
- Week 2 to 4 (Platform integration): Connect the AI layer to Brightree or NikoHealth via API. Map claim fields, order record fields, eligibility results, and document set fields to the AI review model input.
- Week 3 to 5 (Payer rule configuration): Configure payer-specific LCD rules, modifier requirements, PA requirement lists, and denial risk thresholds for the top 10 payers by claim volume.
- Weeks 4 to 6 (Correction queue setup): Configure error type routing queues (modifier queue, documentation queue, PA queue, and eligibility queue). Assign staff to each queue. Define correction SLAs and escalation paths.
- Week 5 to 7 (Parallel run): AI review runs on all claims alongside the existing scrubber. AI error flags are reviewed by staff but do not block submission during the parallel run. This validates that the AI is flagging real errors rather than false positives before it takes on a gatekeeping role.
- Week 7 to 8 (Full deployment): AI review is set to block submission for claims above the denial risk threshold or with confirmed errors. Manual scrubber review is reduced to exception cases. The denial pattern learning loop is activated.
What Are the Limitations of AI Claims Error Detection?
AI pre-submission review reduces preventable denials significantly. It does not eliminate them. Understanding where the technology falls short is as important as understanding what it does well.
1. Clinical Content Quality Is Beyond AI’s Scope
AI can confirm that a Letter of Medical Necessity is present in the order record, is signed, and is dated within the acceptable range. It cannot determine whether the clinical content of that LMN meets the payer’s medical necessity criteria for the specific patient’s condition.
A technically complete but clinically insufficient LMN will pass AI pre-submission review and still generate a denial on medical necessity grounds. Clinical documentation quality remains a human responsibility.
2. Medicare Advantage Plan Rules Require Ongoing Configuration
Each Medicare Advantage plan maintains its own HCPCS coverage policies, PA thresholds, and modifier requirements.
These change annually and sometimes mid-year. An AI pre-submission system is only as current as its MA plan rules configuration. If an MA plan updates its coverage policy in October and the AI configuration is not updated until the next annual refresh, claims billed under the old rules will generate denials that the AI should have caught. Maintaining the current MA plan rules configuration is an ongoing operational requirement, not a one-time setup task.
3. Novel Denial Patterns Take Time to Learn
The learning loop that improves AI denial prediction accuracy requires volume. A new payer, a newly added equipment category, or a newly enrolled referring provider generates claim patterns the AI has not seen before.
In these cases, AI denial prediction accuracy is lower than for established payer-code combinations, and human review of those claims is more important until the model has accumulated sufficient data.
4. False Positives Create Their Own Cost
If the denial risk threshold is set too conservatively, the AI will route too many claims to the correction queue, including claims that would have paid on first pass without correction. This creates staff costs and delays submission without a corresponding denial reduction benefit. Setting the right threshold requires a calibration period using real claim data, which is why the parallel run phase is not optional.
5. AI Review Does Not Replace Post-Submission Denial Management
AI pre-submission review reduces the volume of denials entering the post-submission denial management workflow. It does not handle the denials that do occur; appeals still need to be written, submitted, and tracked. The combination of AI pre-submission review and structured denial management produces better results than either alone.
Frequently Asked Questions
How Does AI Reduce Healthcare Claim Denial Rates?
AI reduces denial rates by catching the errors that cause denials before the claim reaches the payer, rather than after. Traditional claim scrubbers catch formatting and structural errors. AI pre-submission review catches contextual errors, modifier mismatches, PA coverage gaps, documentation holes, and and payer-specific denial risk patterns that scrubbers consistently miss. For DME operations, the combination of AI review and real-time eligibility verification typically reduces first-pass denial rates from 15 to 18 percent to 7 to 10 percent within 6 to 12 months of implementation, per HFMA DME benchmark cohort data.
What Is the Difference Between AI Claims Review and a Claim Scrubber?
A claim scrubber is a rules-based system that checks a claim against a fixed set of edit rules: valid NPI format, valid code combinations, and required fields present. It checks the claim in isolation and does not learn from denial patterns. AI pre-submission review checks the claim in context against the patient's eligibility results, PA on file, document set, payer LCD, and historical denial pattern for this payer-code combination. AI review catches judgment-level errors that scrubbers miss. Both tools are needed. They operate at different layers of the claims workflow.
Does AI Claims Review Work for DME Specifically?
Yes, and DME billing is one of the highest-value use cases for AI pre-submission review because DME denial rates are nearly double the healthcare average and the majority of DME denials are preventable at the pre-submission stage. DME-specific features that AI review must handle include HCPCS Level II code and modifier validation, rental versus purchase rule checking, capped rental month tracking, CMS prior authorization program requirements for power mobility devices and other categories, and Medicare Advantage plan-specific coverage rules. Not all AI claims review tools have been configured for DME-specific billing complexity.
How Long Does It Take for AI Claims Review to Reduce Denial Rates?
Measurable denial rate reduction typically appears within 30 to 60 days of full deployment, once the correction queue is active and claims with flagged errors are being corrected before submission. The most significant improvement occurs in the first 90 days as the correction queue workflow is calibrated and staff become efficient at resolving the most common flagged error types. Further improvement continues over 6 to 12 months as the denial risk model accumulates payer-specific pattern data and the false positive rate decreases.
Is AI Claims Processing HIPAA Compliant?
AI claims processing tools handle PHI at every stage. HIPAA compliance requires a signed Business Associate Agreement (BAA) with the AI platform vendor, SOC 2 Type II certification from infrastructure providers, encryption at rest and in transit, and US-only data residency for PHI storage. HHS HIPAA guidance for healthcare technology vendors outlines the requirements in detail. AWS Bedrock, used by many healthcare AI vendors, supports HIPAA-eligible configurations when a BAA is in place with Amazon.
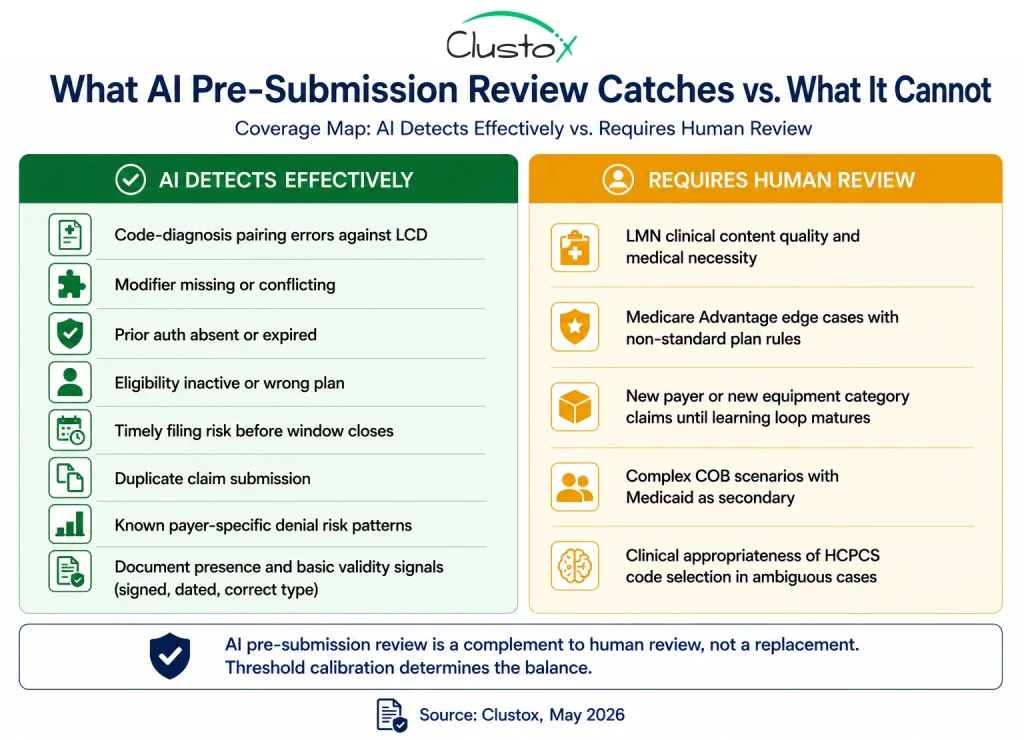
Can AI Catch Every Type of Claims Error?
No. AI pre-submission review is most effective for structured, detectable errors: code-diagnosis pairings, modifier completeness, PA coverage, eligibility status, timely filing risk, and known payer-specific denial patterns. It cannot assess the clinical quality of documentation, cannot resolve Medicare Advantage edge cases without up-to-date plan rules configuration, and produces lower accuracy for new payer-code combinations where the learning loop has not yet accumulated sufficient data. It is a high-value tool with real limits, and those limits should be understood before deployment.
How Does AI Claims Review Integrate With Brightree?
AI pre-submission review connects to Brightree via its published REST API. The AI agent reads the claim record, order data, eligibility results, PA status, and document set from Brightree, runs the pre-submission analysis, and either releases the claim for submission or routes it to a correction queue in Brightree's workflow engine. All AI review decisions are logged in the Brightree audit trail. Brightree's API documentation and integration partner resources are available for development planning. The same integration pattern applies to NikoHealth using its REST API and webhook architecture.
What Is the Right Next Step for Healthcare Operations That Want Fewer Claim Denials?
Healthcare claim denials are rarely random. Most begin with small errors that should have been caught before the claim was ever submitted: missing modifiers, expired prior authorizations, unsupported diagnosis pairings, or incomplete documentation. The cost of fixing those errors after denial is significantly higher than preventing them at the start of the workflow.
AI pre-submission review shifts denial prevention earlier in the revenue cycle. Instead of discovering problems weeks later through ERA rejections, healthcare and DME organizations can identify high-risk claims before submission, reduce preventable denials, improve clean claim rates, and lower the amount of staff time spent on rework.
The technology is not a replacement for human expertise, especially in complex medical necessity and Medicare Advantage scenarios. But for healthcare operations struggling with high denial rates and manual claims review processes, AI-assisted claims validation is quickly becoming one of the most practical and measurable revenue cycle improvements available today.