What this article covers
Clinical documentation software for DME providers automates the capture, storage, and submission of patient records, letters of medical necessity (LMNs), and prior authorization packets. Manual documentation creates avoidable claim denials, audit exposure, and billing delays that reduce revenue. This article explains exactly where the revenue leaks are, what to look for in documentation software, and how to build the case for switching.
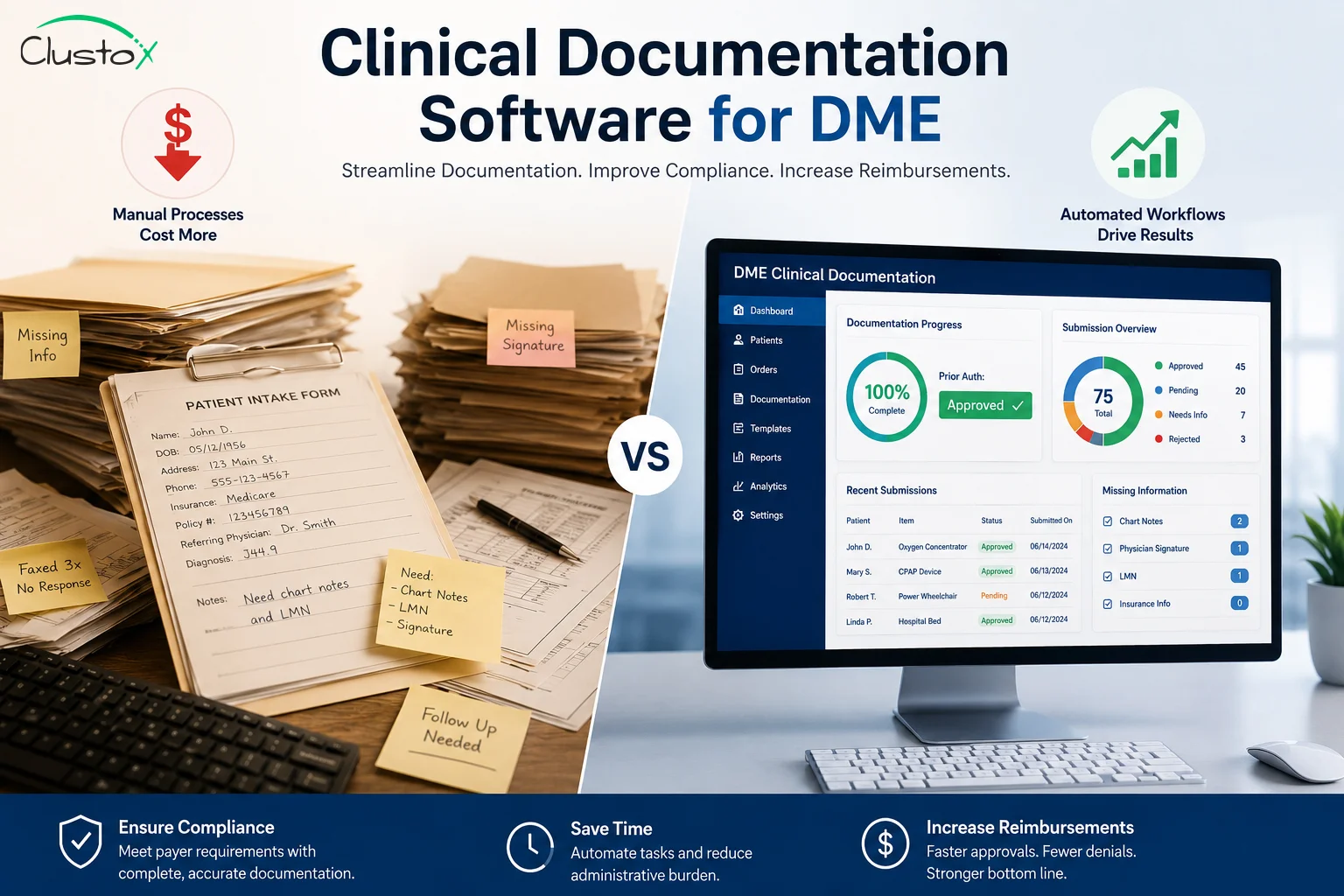
Your billing team submits a claim. It gets denied. The note was incomplete. The LMN did not align with the HCPCS code. Your reimbursement cycle just stretched by 30 to 45 days.
This happens every week in DME practices that rely on manual documentation. It is not a people problem. It is a process problem. And clinical documentation software exists precisely to close that gap.
This guide is for Directors of Billing and Compliance Officers who are tired of chasing down documentation after the fact. You will find out what manual notes actually cost, what good software does differently, and what questions to ask before you buy.
What Is Clinical Documentation Software for DME Providers?
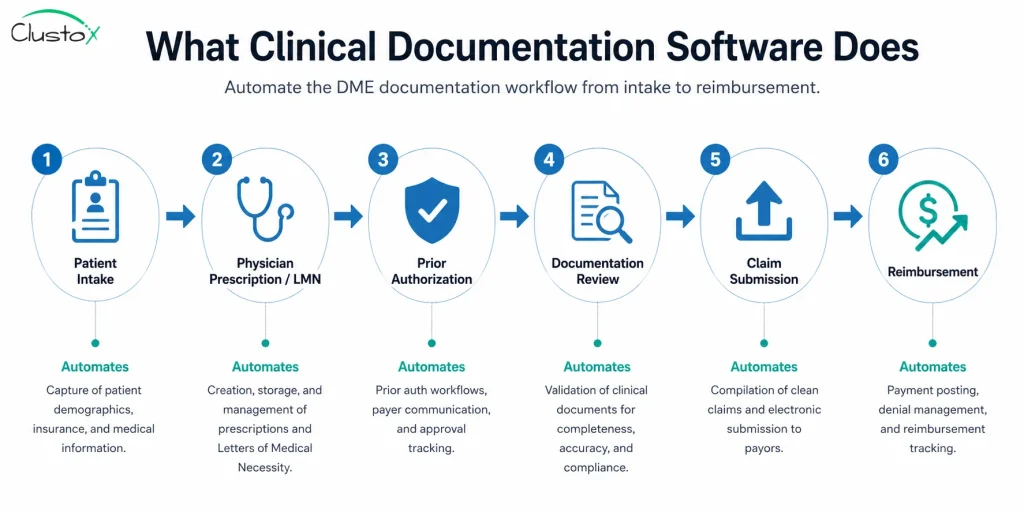
Clinical documentation software is a purpose-built platform that captures, organizes, and manages all clinical records tied to a DME order. That includes patient intake data, prescriptions, LMNs, certificates of medical necessity (CMNs), prior authorization packets, and delivery confirmations.
For DME specifically, documentation is not just an operational detail. It is the foundation of every claim you file. Medicare and most commercial payers require specific clinical evidence before they reimburse. If the documentation does not meet those requirements, the claim fails.
Good clinical documentation software connects your intake workflow directly to your billing platform. When a record is incomplete or missing a required field, the system flags it before the claim goes out, not after.
Table of Contents
How Does Manual Documentation Lead to DME Claim Denials?
Manual documentation fails at the handoff points. A clinician completes a note. A coordinator transcribes it. A biller submits the claim. At each step, information gets dropped, misformatted, or delayed.
The most common documentation-related denial reasons in DME billing include:
- Missing or unsigned LMN
- CMN fields that do not match the ordered HCPCS code
- Incomplete face-to-face encounter documentation
- Prior authorization not obtained before delivery
- Documentation submitted after the timely filing deadline
- Illegible or unsupportable handwritten records during a post-payment audit
Each one of these is a manual process failure. The information existed somewhere. It just was not captured correctly or in time.
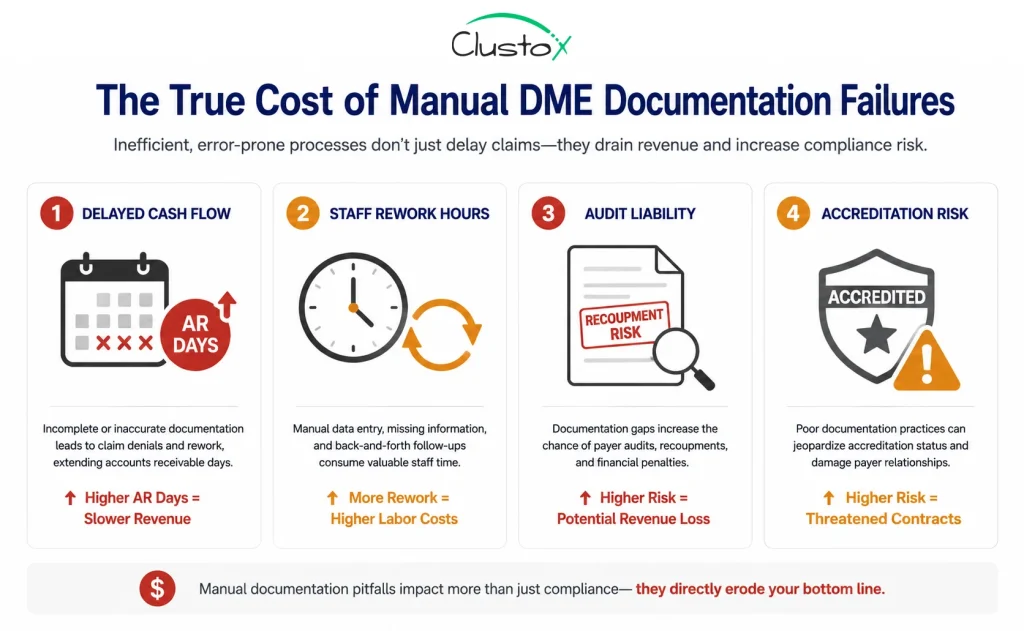
What Does Poor DME Documentation Actually Cost Your Practice?
The direct cost shows up in your denial rate. But the full cost is broader.
Delayed reimbursement cycles
When a claim is denied for documentation reasons, you enter a rework loop. Staff pull the original file, correct the deficiency, and resubmit. That cycle adds weeks to your cash flow timeline. In high-volume practices, the aggregate delay is significant.
Staff time spent on rework
Your billing team spends time on corrections that should not have been necessary. Every hour spent on a rework denial is an hour not spent on proactive follow-up or new claim submission. Manual documentation creates a hidden staffing tax.
Audit liability
CMS and RAC auditors request documentation to verify claims already paid. If your documentation cannot support the claim, you may face a recoupment demand. Incomplete or inconsistent manual records are a direct audit risk.
Accreditation risk
ACHC and BOC accreditation both include documentation standards as part of their review criteria. Practices with weak documentation controls face findings that require corrective action plans.
What Features Should DME-Specific Clinical Documentation Software Include?
Not all documentation platforms are built for DME. Generic EHR systems often lack the specific fields, workflows, and payer integrations that DME billing requires. Here is what to look for.
LMN and CMN template management
Your software should include pre-built, payer-specific templates for LMNs and CMNs. Templates should map directly to HCPCS codes so that required fields are automatically surfaced based on the item being ordered. Freeform notes create inconsistency. Structured templates reduce it.
Prior authorization tracking
Prior authorization management needs to be embedded in the documentation workflow. The system should track auth status, expiration dates, and tie approved auth numbers directly to the claim record. If delivery happens before auth is confirmed, the system should flag it.
Real-time eligibility and documentation validation
Before a claim is submitted, the system should run a completeness check. Does this claim have a valid LMN? Is the face-to-face documentation present? Does the auth number match the payer record? These checks catch denials before they happen.
Integration with DME billing platforms
Your documentation platform needs to talk to your DME billing software. Common DME billing platforms include Brightree, NikoHealth, TIMS, and Universal Software Solutions. Integration eliminates manual data re-entry between the clinical and billing sides of your operation.
Audit trail and document retention
Every record change should be logged with a timestamp and user ID. Audit-ready documentation means you can produce a clean record in response to any payer or compliance request. The system should support the retention periods required under HIPAA and state law.
| Manual Documentation | Clinical Documentation Software |
|---|---|
| LMN completed via fax or handwritten form | Structured digital LMN templates tied to HCPCS codes |
| Prior auth status tracked in spreadsheet | Auth status tracked and linked to claim record in real time |
| Completeness check done manually at submission | Automated validation before claim is submitted |
| Rework requires pulling physical files | Correction and resubmission done within the platform |
| Audit response requires manual document gathering | Audit packet generated automatically from the record |
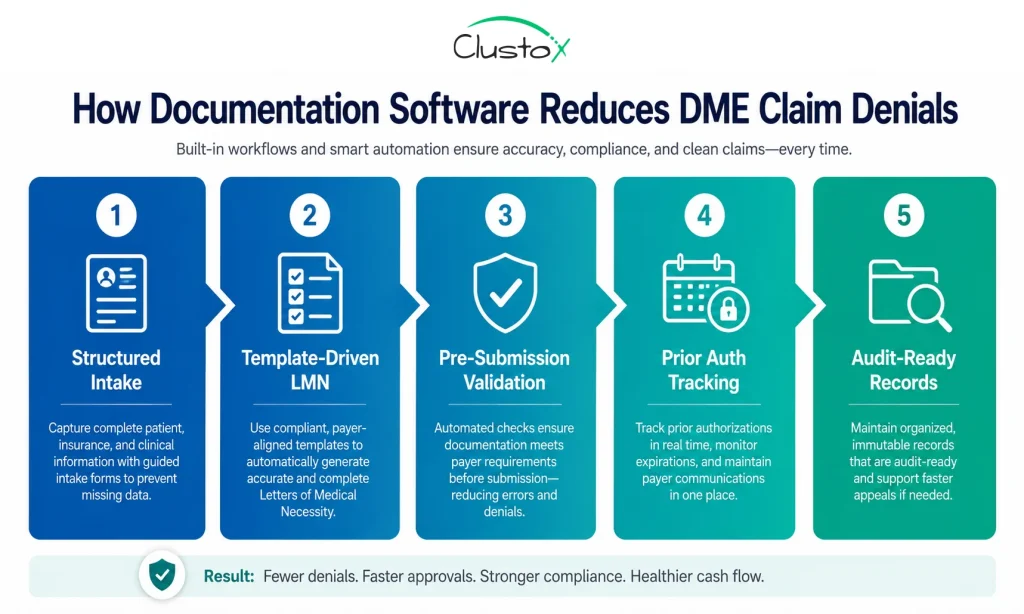
How Does Clinical Documentation Software Reduce DME Claim Denial Rates?
Denial reduction comes from catching errors earlier in the process. Here is how software changes the workflow.
- Structured intake captures required fields at the point of entry. The intake form will not let a coordinator move forward without the fields the payer requires.
- Template-driven LMNs eliminate freeform variation. Every LMN follows the same structure and covers the same required elements.
- Pre-submission validation catches missing or mismatched data before the claim goes out. The system checks the claim against known payer rules.
- Integrated prior auth tracking means your billing team always knows whether authorization is in place before delivery happens.
- Digital records are legible, searchable, and audit-ready. There is no ambiguity about what was documented and when.
How Do You Build the Internal Case for Clinical Documentation Software?
If you are a Director of Billing or a Compliance Officer, you likely already know the problem exists. The challenge is building the business case for leadership.
Here is a framework for structuring that conversation.
Quantify your current denial rate
Pull your denial data by denial reason code. Filter for documentation-related reasons: missing documentation, unsupported services, prior auth not obtained. Calculate the dollar value of those denials over the last 12 months. That number is your baseline.
Calculate your rework cost
Estimate how many staff hours per week are spent on documentation rework and resubmission. Multiply by your loaded labor cost. This gives you an annual cost figure that is easy to present to a CFO or COO.
Assess your audit exposure
If your practice has been subject to RAC or other payer audits, document the recoupment demands and staff time involved. If you have not been audited yet, consider the probability given your claim volume and specialties.
Present the comparison, not just the cost
Decision-makers respond to comparisons. Show what documentation looks like today versus what it looks like with a purpose-built system. Use the feature comparison above as a reference.
Before you select a platform, confirm these items:
-
Does it include LMN/CMN templates specific to your product categories? -
Does it integrate with your current billing platform (Brightree, NikoHealth, TIMS, etc.)? -
Does it include pre-submission claim validation? -
Does it track prior auth status within the same workflow? -
Does it maintain a full audit trail with user IDs and timestamps? -
Does it support HIPAA-compliant document retention? -
What is the implementation timeline, and what does your team’s training look like?
What Should DME Providers Know About HIPAA Compliance in Documentation Software?
Any platform that stores or transmits patient health information must comply with the HIPAA Security Rule and Privacy Rule. When evaluating vendors, confirm the following.
- The vendor will sign a Business Associate Agreement (BAA).
- Data is encrypted at rest and in transit.
- Access controls limit record access to authorized users.
- The system logs all access and modifications.
- The vendor has a documented breach notification process.
HIPAA compliance is not optional, and it is not negotiable. A BAA is the minimum standard for any vendor handling PHI. If a vendor cannot provide one, that is a disqualifying condition.
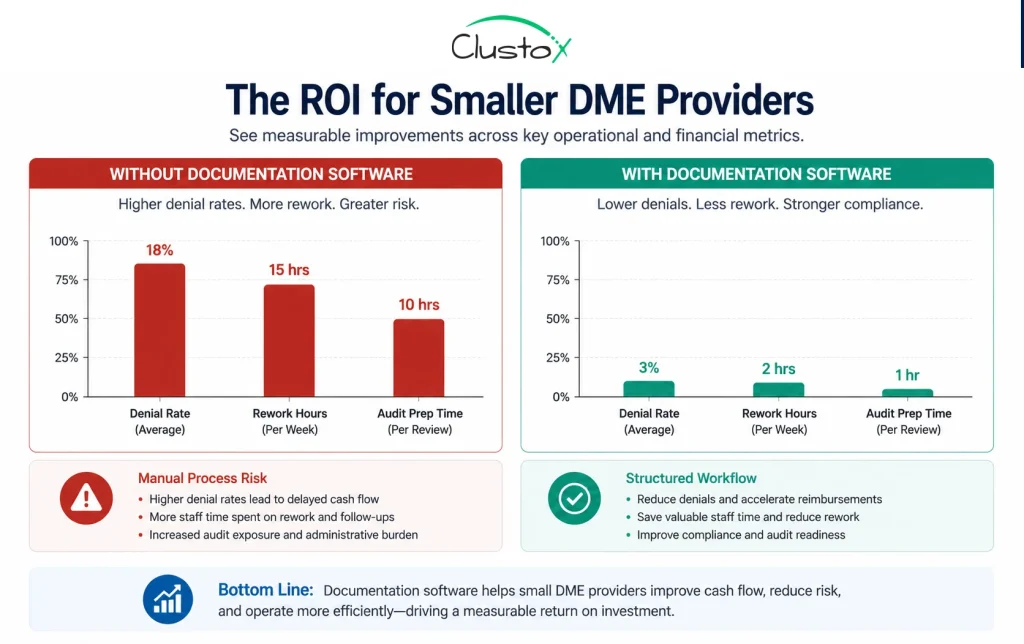
Is Clinical Documentation Software Worth It for Smaller DME Providers?
This is a fair question. Large providers have scale that makes the ROI obvious. For a smaller practice, the calculation is different.
The short answer is: documentation errors cost smaller providers proportionally more, not less. A denial that costs a large provider a rounding error costs a small provider a week of cash flow.
The question is not whether you can afford documentation software. It is whether you can afford the ongoing cost of not having it. For a provider processing 50 or more orders per month, the math usually works.
Evaluate cloud-based, per-user or per-transaction pricing models. Several DME-specific platforms are designed for practices that are not enterprise scale.
Conclusion: Manual Documentation Is a Choice Your Revenue Cannot Afford
Every incomplete note is a delayed payment. Every missing LMN is a potential denial. Every handwritten record is an audit risk.
Clinical documentation software solves a well-defined problem. It structures the information your payers require, validates it before submission, and stores it in a way that survives scrutiny. That is not a technology pitch. That is a revenue protection strategy.
If your denial rate includes documentation-related codes, you already have the business case. The question is how long you want to absorb the cost before you act.
If you are ready to modernize your documentation process, book an audit with Clustox. We combine healthcare workflow expertise with Agentic AI development to help DME providers build faster, more compliant, and audit-ready documentation systems.
Documentation gaps are quietly hurting your cash flow.
Get an expert review of your DME workflow to uncover denial risks, billing inefficiencies, and compliance gaps before they cost you more.
Frequently Asked Questions (FAQs)
Does clinical documentation software integrate with Brightree or NikoHealth?
Many DME documentation platforms offer direct integration with major billing platforms, including Brightree, NikoHealth, and TIMS. The integration avoids manual re-entry of data between clinical and billing workflows. Always confirm the specific integration before selecting a vendor and verify the data fields that transfer automatically.
How does documentation software help with Medicare audits for DME?
The system maintains a complete, timestamped audit trail for every record. When a payer requests documentation to support a claim, you can generate a structured response directly from the platform. The records are legible, organized, and linked to the original claim. That eliminates the scramble that manual documentation creates when an audit request arrives.
Can clinical documentation software reduce prior authorization denials?
It helps significantly. By tracking auth status within the same workflow as the order and documentation, the system prevents delivery before authorization is confirmed. It also stores the auth number directly on the claim record, which eliminates a common submission error. The system will not guarantee an approval, but it closes the workflow gaps that cause avoidable auth-related denials.
How long does it take to implement clinical documentation software for a DME provider?
Implementation timelines vary by platform and practice size. Cloud-based platforms often have shorter onboarding timelines than on-premise systems. A focused implementation typically includes data migration, template configuration for your specific product categories, staff training, and integration setup with your billing platform. Ask vendors for a realistic timeline based on your current system setup.
Is DME documentation software covered under any CMS incentive programs?
DME suppliers are generally not included in the same EHR incentive programs that apply to eligible providers and hospitals under the Medicare and Medicaid EHR Incentive Programs. Evaluate the investment on the basis of revenue recovery and denial reduction rather than incentive eligibility.
Disclaimer
This article is intended for DME providers, operations leaders, and technology decision-makers. It is not medical advice and does not constitute guidance on patient care, equipment selection, or clinical decisions. Regulatory references (CMS, HIPAA, accreditation standards) are accurate as of the review date. Regulations change frequently. Providers should consult primary sources or qualified counsel for current requirements.