
The DME industry is navigating one of its most challenging operating environments in recent memory. The expiration of Medicare’s 75/25 blended reimbursement relief rates led to an average 20% reduction across the top 25 DME HCPCS codes in 2024, according to the American Association for Homecare (AAHomecare).
At the same time, prior authorization requirements continue to expand, payer audits are becoming more aggressive, and staffing shortages remain a persistent challenge across the industry.
In this environment, profitability is no longer determined solely by referral volume or payer contracts. It is increasingly determined by operational efficiency. The DME providers protecting margins in 2026 are not necessarily running larger teams; they are running smarter software stacks.
The best DME software in 2026 combines a proven core practice management platform such as Brightree or Niko-to-end, or comparable solutions, with an Agentic AI layer that automates prior authorization, eligibility verification, denial management, patient outreach, and resupply workflows end-to-end.
This shift is changing how leading DME providers operate. Tasks that once required hours of manual effort can now be completed in minutes, allowing billing teams to focus on exception handling rather than repetitive administrative work. The result is faster authorizations, fewer denials, improved compliance, stronger patient engagement, and higher revenue capture without proportional headcount growth.
This guide compares the leading DME software platforms based on the criteria that matter most to billing directors, COOs, and operations leaders. It also explains where Agentic AI fits into the modern DME technology stack, what workflows it can automate, and how to evaluate software decisions that directly impact revenue, scalability, and long-term operational performance.
What This Article Covers
- How to evaluate DME software in 2026 against real operational criteria
- Platform-by-platform comparison: Brightree, NikoHealth, TIMS, Bonafide, and Fastrack
- Where Agentic AI fits on top of these platforms and what it actually automates
- Real benchmark numbers from DME operators running AI workflows
- A buyer’s checklist for COOs and billing directors making a platform decision
Why Is DME Software Selection a Revenue Decision Rather Than an IT Decision?
Most DME operators treat software selection as an IT project. It is not. The platform you run determines how many prior auth submissions your team can process per day, how quickly denials are identified and appealed, whether CPAP re-supply orders go out on time, and how your operation responds to a Medicare audit. Every one of those outcomes has a direct revenue number attached.
The operators absorbing reimbursement pressure without proportional headcount growth are doing it with a two-layer stack:
Table of Contents
- A core DME platform for intake, order management, HCPCS coding, billing, and inventory
- An Agentic AI workflow layer that runs prior auth, eligibility checks, denial management, and patient communications on top of that platform
The software decision determines whether your billing team spends eight hours a day on phones, or whether they spend two hours reviewing AI-flagged exceptions. That difference is the margin.
How DME Software Stacks Work in 2026?
In 2026, ‘DME software’ no longer means a single platform. High-performing operations run a layered stack. Understanding each layer prevents you from buying the wrong thing or expecting one tool to do a job that requires two.
Layer 1: Core DME Platform
Handles patient intake, order management, HCPCS coding, inventory management, and billing submission. Brightree and NikoHealth dominate this layer. TIMS, Bonafide, and Fastrack serve specific segments. This layer is where your data lives and where your billing team works every day.
Layer 2: Payer Connectivity
Manages EDI transaction handling, eligibility queries (270/271), claim submission (837), and remittance (835). Most major platforms have this built in, but coverage quality varies by payer and plan type. Some platforms connect directly; others route through clearinghouses such as Change Healthcare or Availity.
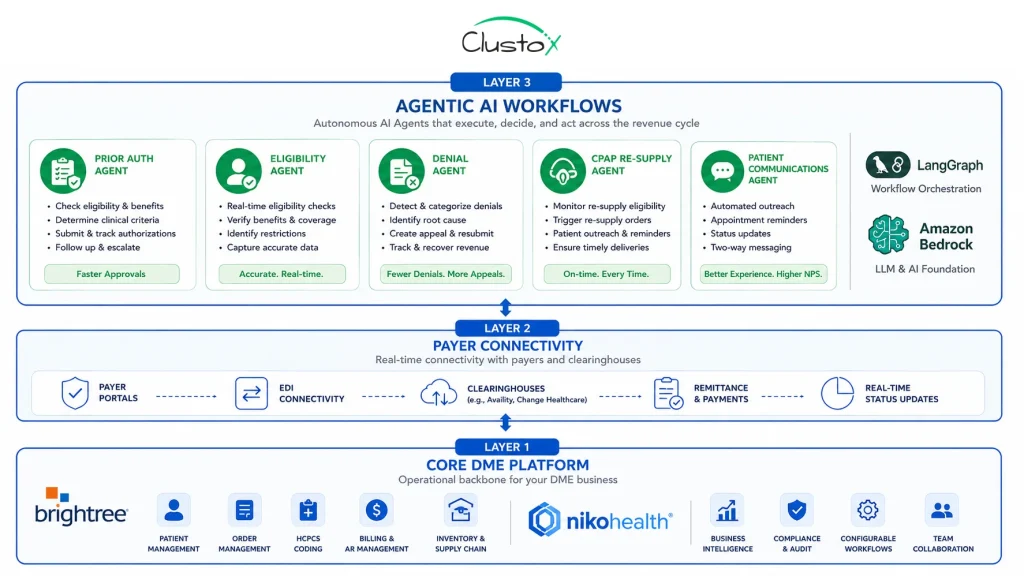
Layer 3: Agentic AI Automation
This is where 2026 looks meaningfully different from 2022. Agentic AI workflows built on frameworks such as LangGraph and deployed on HIPAA-compliant infrastructure such as AWS Bedrock sit on top of Layers 1 and 2 and automate the tasks that previously required staff time on every single order:
- Prior authorization submission, follow-up, and escalation
- Real-time eligibility and benefits verification at multiple points in the order lifecycle
- Denial classification, appeal drafting, and automated resubmission
- CPAP re-supply outreach via voice and SMS agents
- Documentation completeness checks against LMN requirements and payer policy
The platforms in Layer 1 do not provide this level of automation natively. That is the gap that purpose-built Agentic AI solutions fill.
Platform Comparison: Best DME Software in 2026
Each platform below is assessed on the criteria that determine operational performance, not on marketing positioning. No platform is the right answer for every operation. The goal is to match the platform to your current size, payer mix, and AI readiness.
1. Brightree
Best for: Mid-to-large DME providers with complex billing operations, high prior auth volume, and established Brightree workflows.
Brightree, owned by ResMed since 2016, is the market-leading DME platform for providers doing $10M or more in annual revenue. Its strength is breadth: order management, billing, inventory, resupply, and reporting are all native. Its API and integration ecosystem make it the most AI-augmentation-ready platform currently in the market for large operations.
What Brightree Does Well:
- End-to-end order lifecycle from referral intake through remittance processing
- Native resupply automation for CPAP and oxygen patients, though basic relative to AI-augmented versions
- Deep Medicare and Medicaid payer connectivity across commercial plans
- Granular reporting at the department, payer, and product category level
Where Does Brightree Fall Short in Isolation?
- Prior authorization workflows require significant manual touchpoints; automation is rules-based, not AI-driven
- Denial management is reactive; claims are worked after denial, not predicted or prevented
- Patient outreach is limited to basic notification triggers without intelligent channel selection
Brightree is the right foundation for large operations. It is not a complete AI strategy on its own.
Pricing: Contact sales. Typically structured as a percentage of collections or a monthly platform fee. Annual contracts are standard.
2. NikoHealth
Best for: Growth-stage and mid-market DME providers who need a modern interface, faster implementation timelines, and cleaner API access for AI integration.
NikoHealth is the fastest-growing Brightree alternative in the DME space. Built cloud-native, unlike Brightree’s legacy architecture, it offers a cleaner user experience, faster onboarding timelines, and REST API access, making Agentic AI integration substantially easier and less expensive. AAHomecare has recognized NikoHealth as a preferred vendor for independent DME providers.
What Does NikoHealth Do Well?
- Modern UI that reduces staff training time and intake processing errors
- REST API architecture that enables faster Agentic AI integration compared to Brightree’s older API layer
- Transparent SaaS pricing with no percentage-of-collections model
- Strong ACHC and BOC documentation support for accreditation compliance
Where Does NikoHealth Fall Short in Isolation?
- Smaller payer network relative to Brightree for complex Medicare Advantage plans
- Fewer out-of-the-box third-party integrations compared to the Brightree ecosystem
- Less mature reporting for large multi-location operators with complex billing structures
NikoHealth is the right foundation for providers building an AI-first stack from scratch or migrating away from legacy systems. Its API architecture makes the AI layer faster and cheaper to implement.
Pricing: Monthly SaaS pricing with transparent tiers based on user count and feature set.
3. TIMS (Formerly Computers Unlimited)
Best for: Providers with complex inventory management needs, particularly oxygen and respiratory equipment-heavy operations.
TIMS has maintained a loyal customer base among respiratory and home oxygen providers for decades. Its inventory management and delivery routing capabilities are strong. However, its technology architecture is significantly older than NikoHealth’s, and its API integration surface is limited, which makes Agentic AI augmentation more complex and expensive to implement.
For providers whose primary constraint is inventory accuracy and delivery logistics, TIMS remains viable. For providers whose constraint is billing throughput or denial recovery, TIMS creates friction in the AI integration layer.
4. Bonafide
Best for: Smaller DME providers under $3M in revenue seeking an affordable, compliance-focused platform with basic billing functionality.
Bonafide is purpose-built for smaller, single-location providers and focuses on CMS compliance documentation. It handles basic order management and billing submission but lacks the API depth needed for advanced AI integration. Providers who outgrow Bonafide typically migrate to NikoHealth or Brightree.
5. Fastrack
Best for: Niche-segment providers in complex rehab technology (CRT) and wheelchair/mobility equipment categories.
Fastrack has strong HCPCS coding support for complex rehab categories (K0800–K0899 range) and solid payer connectivity for CRT-specific Medicare billing. It is not a general-purpose DME platform.
Providers running mixed product lines typically use Fastrack alongside a secondary system, which creates integration complexity that works against AI implementation.
Side-by-Side Platform Comparison Table
| Criteria | Brightree | NikoHealth | TIMS | Bonafide | Fastrack |
|---|---|---|---|---|---|
| Best for | Large/complex ops | Growth-stage / AI-first | Oxygen / respiratory | Small providers | CRT / mobility |
| API architecture | Older, capable | Modern REST | Limited | Minimal | Limited |
| AI integration difficulty | Medium | Low | High | Very high | High |
| Prior auth automation (native) | Rules-based | Rules-based | Manual | Manual | Manual |
| Denial management (native) | Reactive | Reactive | Manual | Minimal | Minimal |
| CPAP resupply | Strong (native) | Capable | Limited | No | No |
| Medicare Advantage connectivity | Strong | Growing | Moderate | Basic | Basic |
| Implementation timeline | 3–6 months | 6–10 weeks | 4–8 months | 4–6 weeks | 3–5 months |
| Pricing model | % collections or flat | SaaS flat | Flat license | Low flat | Flat license |
How Are AI-First DME Providers Gaining a Competitive Advantage in 2026?
The software platform matters. But the operators pulling ahead in 2026 are not doing it because they chose Brightree over NikoHealth or vice versa. They are doing it because they added an Agentic AI layer that handles the work no DME platform does natively.
Here is what that looks like across four core workflows.
1. Prior Authorization: From 6+ Days to Under 48 Hours
Manual prior authorization for DME gathering documentation, submitting to payer portals, following up on pending requests, and handling peer-to-peer escalations takes the average billing team 6 to 9 days per complex order, according to HFMA’s 2024 Revenue Cycle Benchmarking Report.
An Agentic AI prior authorization workflow integrated with Brightree or NikoHealth handles this differently:
- Pulls the order, LMN, and clinical documentation automatically from the core platform
- Checks payer-specific PA requirements against current CMS and Medicare Advantage policy
- Submits via payer portal or fax API with zero manual data entry
- Monitors for status updates and auto-escalates stalled requests to a human reviewer
Operators running this configuration report prior auth turnaround dropping from 6+ days to under 48 hours for standard HCPCS categories including E0601 (CPAP devices) and E1390 (oxygen concentrators). The same billing team handles two to three times the order volume without additional headcount.
2. Eligibility Verification: Eliminating the ‘Verified but Still Denied’ Problem
Eligibility verification failure is one of the leading causes of soft denials in DME billing. A patient who verified as covered at intake may have had a plan change, a benefit exhaustion, or a coordination-of-benefits issue by the time the claim drops, especially for recurring CPAP supply orders or ongoing oxygen recertifications.
AI-powered eligibility verification agents run real-time 270/271 checks at three points in the order lifecycle: at intake, at PA submission, and at claim drop. They also flag benefit-limit proximity, for example, ‘patient is at 85% of annual E1390 benefit,’ and route exception cases to a human reviewer before the claim goes out wrong. Providers implementing multi-point eligibility verification report soft denial rates dropping by 15 to 22%.
3. Denial Management: Recovering Revenue Most Teams Write Off
The average DME provider writes off 6 to 12% of submitted claims as unrecoverable, according to OIG’s 2023 DME billing compliance report. Most of those write-offs are soft denials, claims denied for documentation gaps, authorization mismatches, or coding errors that are correctable on appeal.
Agentic AI denial management classifies every denial by type and root cause: missing LMN, incorrect HCPCS modifier, or prior authorization mismatch; timely filing drafts the appropriate appeal with supporting documentation and submits it within the payer’s appeal window automatically.
It also feeds denial patterns back upstream to prevent the same error on future claims. DMEs using this workflow recover 18 to 27% of previously written-off soft denials within 90 days of implementation.
4. CPAP Re-Supply: Voice and SMS Agents That Drive Real Compliance Revenue
CPAP re-supply is a high-margin, high-volume revenue stream and it leaks constantly through patient non-response. A patient who does not answer the phone or respond to a paper mailer does not get their supplies reordered. That is lost revenue for the provider and a compliance risk for the patient.
AI voice agents and SMS agents handle outbound re-supply outreach at scale: contacting patients on their preferred channel, confirming supply needs, capturing refusal or deferral, and pushing confirmed re-orders back into Brightree or NikoHealth for fulfillment.
No billing coordinator time required for routine outreach. Providers running AI re-supply outreach report a 30 to 40% improvement in monthly re-supply order capture compared to phone-only outreach.
What Results Are DME Providers Seeing From Agentic AI Implementations?
The following benchmarks reflect Clustox implementations across DME clients running Brightree and NikoHealth. Results vary based on payer mix, order volume, and existing workflow maturity.
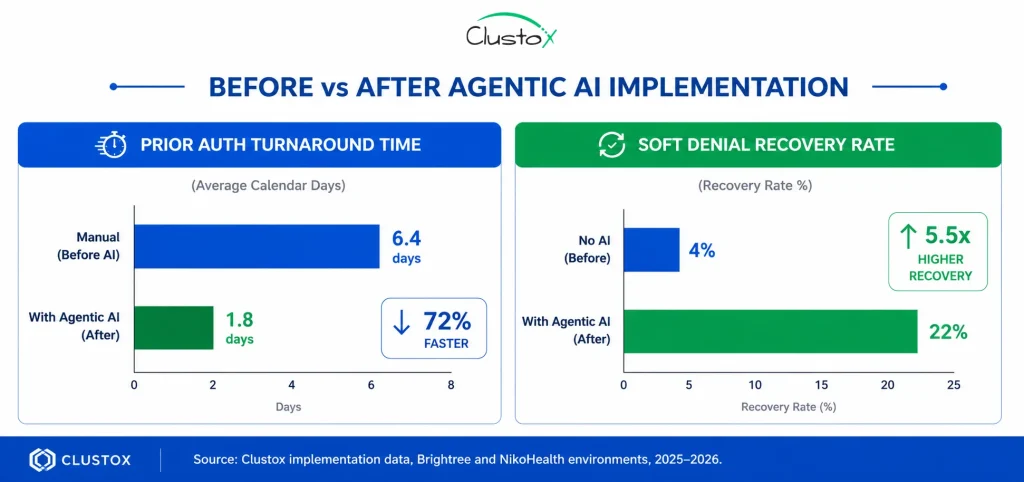
- Prior auth turnaround time: 6+ days (manual) reduced to under 48 hours (AI-automated) for standard HCPCS categories including E0601 and E1390
- Soft denial recovery: 18–27% of previously written-off denials recovered within 90 days
- CPAP re-supply capture: 30–40% improvement in monthly order volume
- Eligibility-driven soft denials: reduced by 15–22% with multi-point verification
- Billing team capacity: same headcount handling 2–3x order volume after prior auth and eligibility automation
What Are the Biggest Challenges and Limitations of Agentic AI in DME Operations?
Agentic AI in DME operations is delivering real results, but it is not a zero-configuration solution. Here is what current implementations still get wrong and what to watch for before you commit.
1. Payer Portal Inconsistency
Some Medicare Advantage plans have non-standard PA portal interfaces that do not expose consistent API endpoints. AI agents that work cleanly on a UnitedHealthcare portal may require a manual fallback for a regional MA plan. This is improving as clearinghouses standardize, but it is not fully solved.
2. LMN Quality Variability
AI can check whether a Letter of Medical Necessity is present and whether it contains required elements, but it cannot fix a poorly written LMN from a referring physician. Providers with weak referral source relationships see higher PA denial rates regardless of automation quality.
3. Complex Rehab and Custom Equipment
Agentic AI automation works most cleanly for high-volume, standardized product categories such as CPAP, oxygen, and standard wheelchairs. For CRT, custom orthotics, or custom power wheelchairs (K0800–K0899), documentation complexity and payer-specific policy variation still require skilled human oversight.
4. Multi-System Environments
Providers running TIMS alongside a secondary system and manual spreadsheet layers have significantly higher AI integration costs and longer implementation timelines than those on a single modern platform. The AI layer is only as clean as the data layer beneath it.
5. RAC and TPE Audit Response
AI can help organize documentation packages for TPE (Targeted Probe and Educate) or RAC audit responses, but these processes still require human review and legal awareness. Do not automate audit responses without a qualified reviewer in the loop.
Buyer’s Checklist: Evaluating DME Software in 2026
Use this before making a platform decision or signing a contract extension. These are the questions that separate a good evaluation from one you will regret.
- API access quality. Can you get a REST API with full read/write access to orders, claims, and patient records? If the answer is ‘only through a third-party integration partner,’ your AI implementation costs double.
- Prior auth workflow configurability. Can you define custom PA workflows by payer and product category, or is it a fixed, rules-based flow you cannot modify?
- Eligibility check frequency. Does the platform support multiple eligibility checks per order at intake, PA submission, and claim drop or only once at intake?
- Denial data export. Can you pull denial data in a structured format (CSV, JSON, or API) for analysis and AI training, or is it locked in a non-exportable reporting view?
- Resupply automation depth. For CPAP and recurring supply products, does the platform support outbound voice and SMS outreach, or only internal notifications?
- HIPAA compliance architecture. Is the platform HIPAA BAA-eligible with your AI infrastructure provider AWS Bedrock, Azure, or GCP? This is non-negotiable.
- Implementation timeline and migration support. What is the realistic go-live timeline including data migration? Get it in writing, with penalty clauses for delay.
- Audit trail and documentation. Does the platform maintain a complete audit trail for every prior auth submission, eligibility check, and claim action? This is essential for TPE and RAC audit defense.
Frequently Asked Questions
How does Agentic AI differ from the automation already built into Brightree or NikoHealth?
Native automation in Brightree and NikoHealth is rules-based: if X, then Y. It handles predictable, structured workflows. Agentic AI is goal-directed: it can navigate payer portals, handle exceptions, draft appeals, and manage multi-step processes that require judgment without human input on the majority of cases. The two are complementary, not competing.
Can I add AI on top of my existing DME platform, or do I need to switch platforms first?
In most cases you can add an Agentic AI layer on top of your existing platform without switching. If you are on Brightree or NikoHealth, AI integration is straightforward. If you are on TIMS or an older legacy system, integration is more complex and may require a platform migration as part of the AI project. A 48-hour AI Readiness Audit will tell you the realistic cost and timeline before you commit.
Which HCPCS categories benefit most from AI prior auth automation?
High-volume, standardized categories with clear CMS coverage criteria: E0601 (CPAP devices), E1390 (oxygen concentrators), L0650-L0651 (prefabricated cervical orthoses), and K0001-K0108 (standard and lightweight wheelchairs). Complex categories K0800-K0899 (power wheelchairs, CRT) benefit from AI assistance but still require human review for non-standard cases.
Is AI-driven DME billing HIPAA compliant?
It can be, but it requires deliberate architecture. All AI processing of PHI must occur within a HIPAA Business Associate Agreement with the infrastructure provider. AWS Bedrock, Azure OpenAI, and GCP Vertex AI all offer BAA-eligible environments. HIPAA compliance is not a feature of an AI model; it is an architecture requirement that must be designed in from the start.
How long does it take to implement an AI layer on top of Brightree?
A focused Agentic AI implementation for prior auth and eligibility on Brightree typically takes 8 to 12 weeks from signed contract to live workflow, assuming API access is in place and documentation is available. Denial management adds 4 to 6 weeks. CPAP voice and SMS outreach agents add 3 to 4 weeks. Timelines extend if data cleanup or platform migration is required.
What is the ROI timeline for DME AI software investment?
Most providers see measurable ROI within the first billing cycle post-implementation typically 30 to 60 days through recovered soft denials alone. Prior auth acceleration shows in operational metrics within 30 days. CPAP re-supply revenue uplift shows in the first re-supply cycle post-deployment.
Does switching DME platforms disrupt AI integration plans?
Yes, if not sequenced correctly. If you are migrating platforms and building an AI layer simultaneously, the integration work will need to be redone after migration. The better sequence: migrate first, stabilize on the new platform, then implement the AI layer. Alternatively, audit your current platform's AI integration feasibility before committing to a migration you may not need to switch.
What is the difference between a DME software vendor's built-in AI and a purpose-built Agentic AI workflow?
DME platform vendors are beginning to market 'AI features' typically copilots, coding suggestions, or basic workflow flags. These are single-function tools. Purpose-built Agentic AI workflows are multi-step, goal-directed systems that handle full prior auth cycles, denial appeals, and patient outreach end to end without human input on routine cases. Ask vendors to demonstrate a complete prior auth cycle from order creation to payer approval with no manual touchpoints.
How do I know if my operation is ready for AI implementation?
The key variables are data quality in your core platform, API access availability, billing team readiness to adapt workflows, and leadership clarity on which problem to solve first. A 48-hour AI Readiness Audit maps these variables and produces a prioritized workflow plan with a fixed-cost ROI model before you commit to any implementation spend.
Conclusion
The DME software landscape in 2026 is not complicated to read once you understand what each layer does. Brightree and NikoHealth are the two platforms worth serious consideration for most operations Brightree for scale and depth, NikoHealth for speed and AI integration. TIMS, Bonafide, and Fastrack serve specific niches and are best evaluated honestly against the integration cost they introduce.
What separates the operators gaining margin from those holding steady is not which core platform they chose. It is whether they added an Agentic AI layer on top of that platform one that handles prior auth end to end, verifies eligibility at every touchpoint, recovers soft denials automatically, and drives re-supply revenue without adding staff. That is the difference between a billing department that processes orders and one that drives revenue.
The path forward is straightforward: assess your current platform’s AI integration feasibility, identify the two or three workflows that generate the most friction or write-offs, and build the AI layer there first. Most operations recover the cost of implementation within the first 60 days through denial recovery alone.
If you are not sure where to start, that is exactly what the AI Readiness Audit is built for.