Every DME order begins with a question: Is this patient covered, and does their plan cover this specific equipment?
The method used to answer that question determines how long it takes to intake, how accurate the answer is, and how many claims get denied because the answer was wrong.
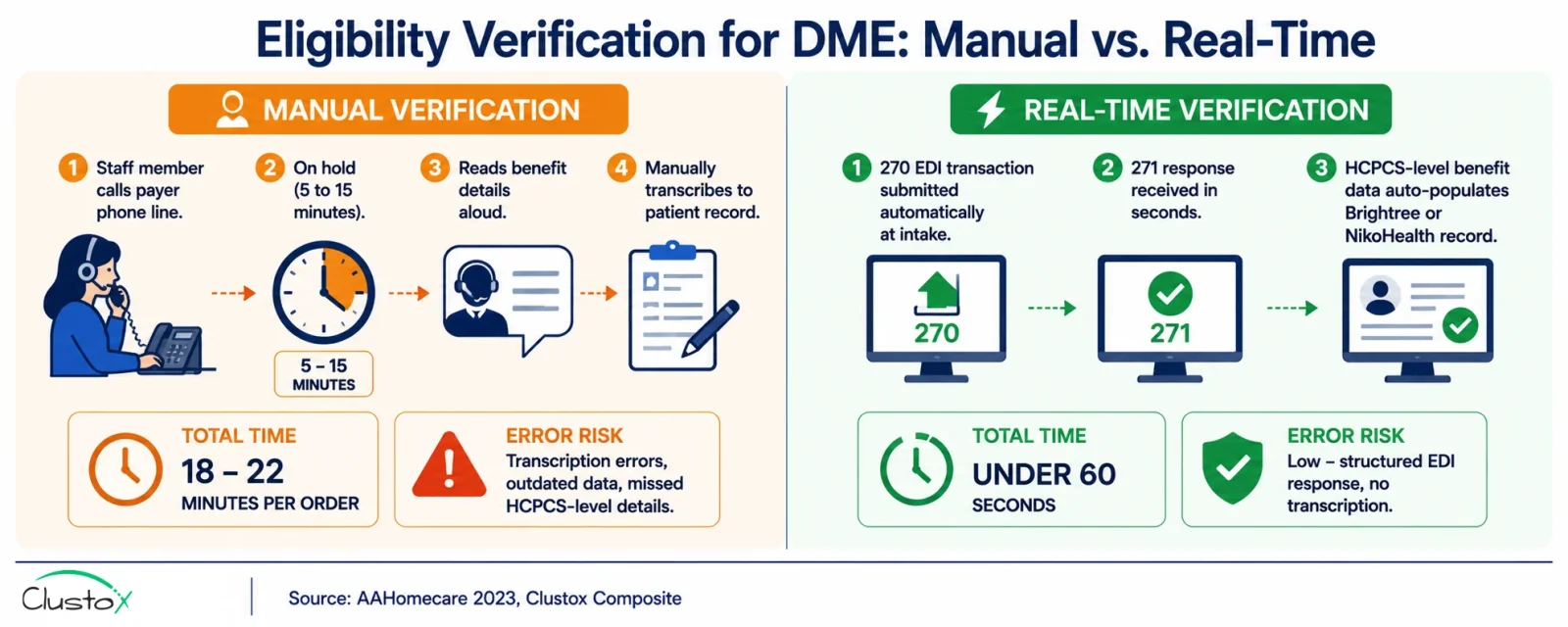
Manual eligibility verification averages 18 to 22 minutes per order, including a phone call to the payer, time on hold, a manual read of the benefit details, and a handwritten or typed note in the patient record.
For a DME operation processing 300 orders per month, that is more than 100 staff hours spent on a task that produces no direct value, only risk management. And it still generates errors: transcription mistakes, outdated coverage data, and missed HCPCS-level benefit details that cause claims to deny weeks later.
According to AAHomecare’s 2023 Operational Survey, eligibility errors are the second-leading cause of DME claim denials, accounting for approximately 22 percent of denials across the industry.
Real-time eligibility verification eliminates the phone call. An automated agent submits a 270 EDI transaction to the payer and receives a 271 response with active coverage status, HCPCS-level benefit details, deductible balance, PA requirements, and rental versus purchase rules in seconds.
The data populates the patient record in Brightree or NikoHealth automatically. No call, no hold time, no transcription. The CMS 2023 Medicare Fee-for-Service Improper Payment Data attributes more than 1.2 billion dollars annually in DME improper payments to eligibility and errors, age errors, the majority of which are detectable at the point of intake with real-time verification.
The comparison between real-time and manual eligibility verification is not primarily a technology question. It is an operational and financial one: what does each method cost per order, what errors does each method introduce, and what is the impact on claim denial rates and staff capacity?
Table of Contents
This guide answers those questions directly.
What Does This Guide Cover?
- What insurance eligibility verification for DME involves and what data it must return
- How manual eligibility verification works and where it consistently fails
- How real-time 270/271 EDI eligibility verification works and what it requires
- Side-by-side comparison across cost, accuracy, denial impact, and speed
- Medicare Advantage eligibility: where real-time verification has limits
- Implementation requirements for connecting real-time eligibility to Brightree and NikoHealth
- Real benchmarks from DME operators across both methods
- Eight frequently asked questions from DME billing directors and intake managers
What Does Insurance Eligibility Verification for DME Need to Confirm?
Insurance eligibility verification for DME goes well beyond confirming that a patient has active coverage. A basic active or inactive check is insufficient for DME billing because coverage status alone does not confirm whether the specific equipment is covered, under what billing rules, or with what patient financial responsibility.
A complete DME eligibility check must return the following eight data elements before an order qualifies for fulfillment.
1. Active Coverage Status on the Date of Service
The patient’s coverage must be confirmed as active on the date the equipment will be delivered, not just on the date the referral was received. Coverage that is active today may lapse before delivery, particularly for patients with employer-sponsored plans during open enrollment periods or benefit transitions.
2. Plan Type Identification
Correct plan type identification is critical because billing rules differ fundamentally across Medicare Part B, Medicare Advantage, Medicaid, and commercial plans. A patient showing Medicare coverage may be enrolled in a Medicare Advantage plan that requires a different billing approach, different PA requirements, and plan-specific HCPCS coverage rules. Billing Medicare Part B for a Medicare Advantage patient generates an automatic denial. CMS Medicare Advantage plan lookup resources provide current plan directories by state.
3. HCPCS-Level Benefit Confirmation
Active coverage status does not mean the specific HCPCS code requested is covered under the patient’s plan. HCPCS-level benefit confirmation checks whether the equipment category, power wheelchair, oxygen, CPAP, hospital bed, or orthotic is a covered benefit under the specific plan and whether any equipment-specific coverage criteria apply.
This is the data element most commonly missed in manual eligibility checks because payer phone representatives frequently provide only active or inactive status and do not volunteer HCPCS-level details unless specifically asked.
4. Deductible Remaining and Copay/Coinsurance Rates
Deductible and cost-sharing data is needed for two purposes: generating an accurate patient financial responsibility estimate at intake and preventing the situation where a claim is filed correctly but returns a lower payment than expected because the patient’s deductible was not yet been met. Patients who are not informed of their financial responsibility before delivery are also more likely to dispute invoices, creating accounts receivable problems that compound.
5. Prior Authorization Requirements
Eligibility verification must confirm whether a prior authorization is required for the equipment category and HCPCS code requested. For equipment covered under the CMS Prior Authorization program for DME, a missing PA is an automatic denial with no appeal path. Manual eligibility checks frequently miss PA requirements because phone representatives do not always flag them proactively.
6. Rental Versus Purchase Rules
Oxygen, CPAP, power wheelchairs, and certain other equipment categories have specific rental versus purchase rules under Medicare, including capped rental provisions that govern how many months the equipment is billed as rental before title transfers to the patient. CMS capped rental billing guidance defines the month-specific billing rules for each equipment category. Billing a capped rental item as a purchase, or miscounting rental months, generates a claim rejection or underpayment.
7. Coordination of Benefits
When a patient has more than one active insurance policy, eligibility verification must identify the primary and secondary payer and establish the billing order before the claim is submitted. Filing with the wrong primary payer generates a denial that requires coordination of benefits to resolve, adding days to the reimbursement cycle.
8. Network Status
For Medicare Advantage and commercial plans, eligibility verification should confirm whether the DME provider is in-network for the patient’s specific plan. An out-of-network status affects patient cost-sharing, may generate different reimbursement rates, and in some cases results in a denial if the plan does not cover out-of-network DME.
How Does Manual Eligibility Verification Work and Where Does It Consistently Fail?
Manual insurance eligibility verification for DME follows one of two approaches: a phone call to the payer’s provider services line or a manual look-up through the payer’s online provider portal. Both approaches are slow, error-prone, and difficult to scale.
1. The Phone Verification Process
A billing coordinator or intake specialist calls the payer’s provider services number, navigates the automated phone system, waits on hold (typically 5 to 15 minutes for Medicare and major commercial payers), reads the patient and provider information to the representative, receives a verbal description of the patient’s benefits, and manually transcribes the relevant details into the patient’s record in Brightree, NikoHealth, or a paper intake form. Total time per check: 18 to 22 minutes on average, per AAHomecare 2023.
2. The Portal Look-Up Process
Some DME operations use payer online portals for eligibility look-ups. This reduces hold time but retains the manual data entry and transcription steps. Staff must log into each payer’s separate portal, search for the patient record, read the benefit summary, and manually enter the relevant fields into the patient record. Portal look-ups typically take 8 to 12 minutes per check faster than phone calls but still representing significant manual effort at scale, and still subject to transcription error.
3. Where Manual Verification Consistently Produces Errors
- Transcription errors: Coverage details communicated verbally or read from a portal screen are frequently transcribed incorrectly. A deductible of 1,850 dollars becomes 1,580 dollars. An in-network copay rate is recorded instead of the out-of-network rate. These errors surface weeks later as underpayments or claim adjustments.
- Incomplete HCPCS-level detail: Phone representatives typically confirm whether a patient has DME benefits but do not volunteer HCPCS code-specific coverage details unless specifically asked. Most intake staff are not trained to ask the right probing questions for each equipment category, resulting in eligibility records that confirm coverage in general but miss equipment-specific coverage restrictions.
- Missed PA requirements: Prior authorization requirements are inconsistently communicated during manual phone verification. Representatives may note that PA is required without specifying the HCPCS code threshold or the specific payer portal for PA submission, leaving the intake team with incomplete information about what needs to happen before the order can proceed.
- Data staleness: Manual eligibility checks are a point-in-time snapshot. Coverage verified on Monday may have changed by Wednesday if the patient’s employer plan updates, the patient enters a new plan year, or a Medicare Advantage plan processes a mid-year coverage change. Without a re-verification step before delivery, manual eligibility checks carry an inherent staleness risk for orders with longer lead times.
- Scale constraints: Manual verification does not scale without adding staff. A 300-order-per-month operation running manual verification needs a dedicated intake team. A 600-order-per-month operation needs a larger one. Staff capacity becomes the ceiling on order volume, which means that revenue growth is directly constrained by headcount.
How Does Real-Time Insurance Eligibility Verification Work for DME?
Real-time eligibility verification for DME uses the ANSI X12 270/271 EDI transaction set to query payer eligibility data electronically and receive a structured response in real time or near real time. The query is submitted automatically at the point of intake, without a staff member initiating it, and the response populates the patient record directly.
1. The 270/271 EDI Transaction Explained
The 270 transaction is the eligibility inquiry. It contains the patient’s member ID, the provider NPI, the date of service, and the service type code for the equipment category requested. The payer receives the 270 and returns a 271 transaction, the eligibility response containing the patient’s coverage status, benefit details, deductible, and cost-sharing information, and any coverage restrictions or PA requirements for the requested service type.
The transaction completes in seconds for payers with real-time 271 response capability. CMS publishes 270/271 transaction implementation guides via the Medicare Learning Network. Clearinghouses, including Availity, Waystar, and Change Healthcare, manage 270/271 routing between the DME provider and the payer.
2. How the Automated Eligibility Agent Works
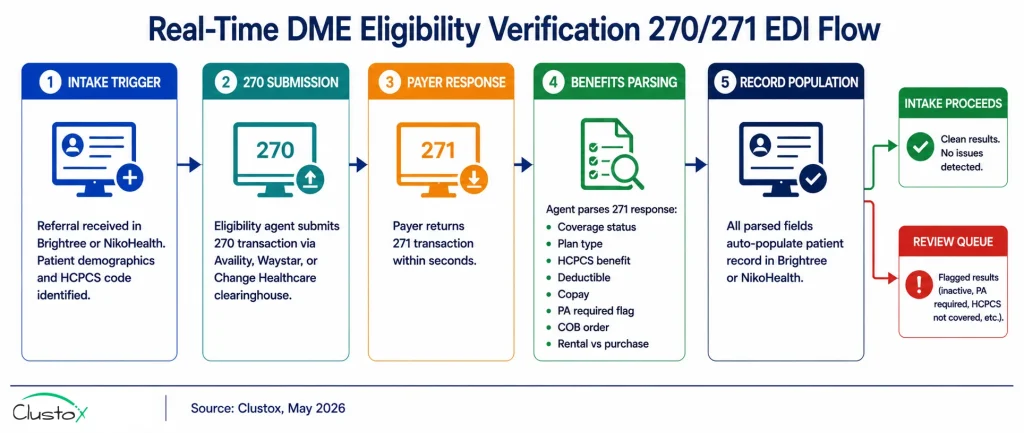
In a fully automated setup, the eligibility agent runs as follows. A new patient referral enters the system through Brightree, NikoHealth, or an intake automation layer. The agent reads the patient demographics, insurance information, and the requested HCPCS code from the intake record. It submits a 270 transaction to the payer via the clearinghouse.
The 271 response is received and parsed: active coverage status, plan type, HCPCS benefit confirmation, deductible remaining, copay and coinsurance rates, PA requirements, rental versus purchase rules, and COB data. All parsed fields populate the patient record automatically. The intake workflow proceeds to the next step, PA routing, documentation collection, or order qualification, without any staff intervention for the eligibility step.
3. What Triggers a Real-Time Eligibility Check?
In a well-configured automated intake workflow, the eligibility check triggers automatically at three points: at referral receipt (to confirm coverage before the order progresses), within 24 to 48 hours of the scheduled delivery date (to confirm coverage has not lapsed), and at each resupply trigger for CPAP, oxygen, and other resupply programs.
The third trigger is particularly valuable for resupply operations, where a lapsed coverage flag returned at delivery rather than at the resupply trigger avoids a shipment that cannot be billed.
4. How Results Are Returned to the Core Platform
Eligibility results are written back to the patient and order record in Brightree or NikoHealth via API. Specific fields populated include coverage status, plan name, member ID confirmed, benefit effective date, deductible remaining, copay rate, PA required flag, HCPCS coverage flag, and COB payer order.
The populated record provides the billing team with the complete benefit picture without any manual steps. Orders with eligibility flags inactive coverage, PA required, HCPCS code not covered route to a defined review queue with the specific flag noted.
How Do Real-Time and Manual Eligibility Verification Compare Across Key Dimensions?
The comparison below covers the six dimensions that matter most to a DME operations director or billing manager making a method decision: time per check, cost per check, data completeness, denial impact, scalability, and accuracy.
1. Time Per Eligibility Check
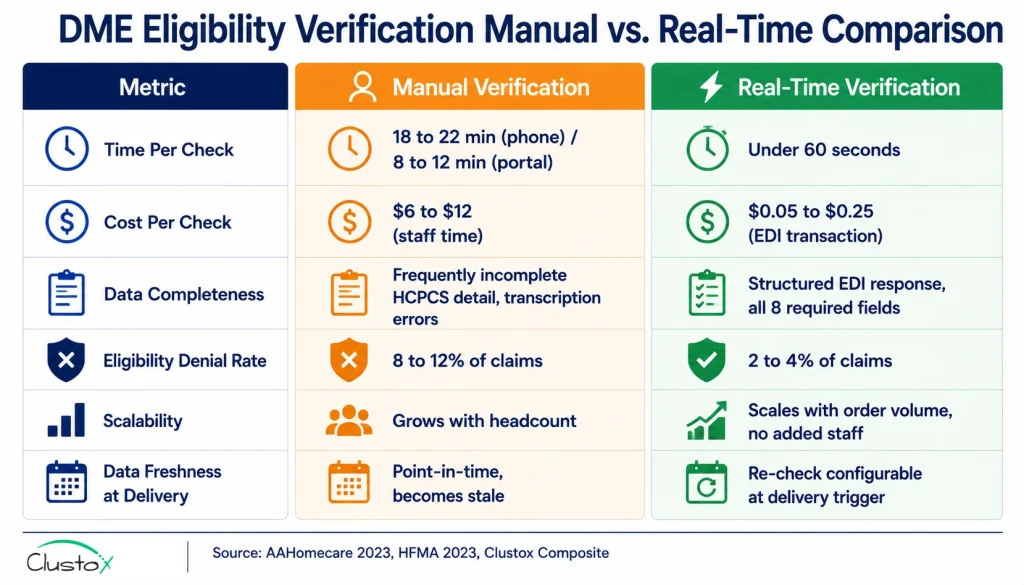
Manual phone verification averages 18 to 22 minutes per order, per AAHomecare’s 2023 Operational Survey. Manual portal look-ups average 8 to 12 minutes. Real-time 270/271 EDI verification returns results in under 60 seconds for payers with real-time 271 response capability. For payers that do not support real-time 271 responses and return batch responses instead, turnaround is typically 2 to 4 hours rather than same-day.
The time saving per order from real-time versus manual phone verification is 17 to 21 minutes. At 300 orders per month, that is 85 to 105 staff hours recovered monthly from a single workflow step.
2. Cost Per Eligibility Check
Manual phone verification costs range from 6 to 12 dollars per check when fully loaded billing coordinator time (22 to 28 dollars per hour) is applied against the 18 to 22-minute average duration. Real-time 270/271 EDI verification costs 0.05 to 0.25 dollars per transaction through a clearinghouse, depending on clearinghouse pricing and contract volume.
At 300 orders per month, the cost difference between manual and real-time verification ranges from 1,750 to 3,500 dollars monthly in staff cost alone, before accounting for the denial reduction value. HFMA attributes eligibility-driven denials to a rework cost of approximately 118 dollars per claim, which the real-time verification cost structure eliminates for the majority of eligibility-caused denials.
3. Data Completeness and Accuracy
Real-time 270/271 verification returns a structured EDI response that covers all eight required data elements: coverage status, plan type, HCPCS benefit, deductible, copay/coinsurance, PA requirements, rental versus purchase rules, and COB data in a machine-readable format that populates directly into the patient record without transcription. Manual verification is subject to incomplete verbal benefit summaries, transcription errors, and phone representative variability in what benefit details are volunteered. HCPCS-level benefit details and PA requirements are the two data elements most frequently missing from manual eligibility records.
4. Denial Rate Impact
Eligibility errors cause approximately 22 percent of DME claim denials, per HFMA DME benchmark cohort data. Operators using real-time eligibility verification with HCPCS-level benefit parsing consistently report eligibility-driven denials falling from 8 to 12 percent of claims to 2 to 4 percent, per Clustox client composite data (2024 to 2025, anonymized). The denial rate improvement is most pronounced for eligibility-related denials but also affects PA-related denials, since the real-time 271 response flags PA requirements that manual checks frequently miss. Total first-pass denial rates for operations using real-time eligibility typically fall from the 15 to 18 percent industry average to 7 to 10 percent when combined with other intake automation, per HFMA DME benchmark cohort data.
5. Scalability
Manual eligibility verification scales with headcount. Each additional 100 orders per month requires approximately 25 to 30 additional staff hours of eligibility verification capacity, which means operational growth requires staffing growth at a consistent ratio. Real-time eligibility verification scales with order volume automatically: 300 orders per month or 3,000 orders per month require the same staff time for the eligibility step, since the agent handles each query without human involvement. Staff time is freed for exception review rather than routine verification.
6. Data Freshness at Time of Delivery
Manual eligibility checks are a point-in-time snapshot that becomes stale as soon as coverage changes. Real-time verification can be configured to re-check automatically at the delivery trigger, confirming that coverage is still active on the delivery date rather than relying on a check that was performed days or weeks earlier at intake. For orders with lead times of more than 48 hours, delivery-point re-verification is a meaningful safeguard against shipping equipment under coverage that has since lapsed.
Where Does Real-Time Eligibility Verification Have Limits for Medicare Advantage?
Real-time 270/271 EDI eligibility verification handles Medicare Part B eligibility well. For Medicare Advantage, the picture is more complicated, and DME operators with significant MA patient volume need to understand where real-time verification has gaps.
Standard 271 Responses May Not Reflect Plan-Specific DME Rules
A standard 271 response from a Medicare Advantage plan confirms that the patient is enrolled in an MA plan and that the plan includes DME benefits. It does not always return the plan-specific HCPCS coverage rules that govern what is actually covered, at what reimbursement rate, and under what PA requirements.
Each of the more than 800 active MA plans in the United States maintains its own coverage policies that can differ significantly from Medicare Part B rules. CMS Medicare Advantage plan resources provide plan-level directories, but HCPCS-specific coverage rules must be obtained directly from each plan.
Plan-Specific Coverage Rules Require a Separate Rules Library
A real-time eligibility system that returns only the standard 271 response for MA patients will confirm that DME benefits exist but will not flag that a specific plan covers power wheelchairs only at a lower PA threshold than Medicare Part B or that another plan requires a different LMN format for oxygen claims.
This gap is why eligibility verification platforms with an actively maintained MA plan rules library updated at least quarterly outperform those relying on standard EDI responses alone for MA patients.
When Manual Verification Still Makes Sense for MA Patients
For MA patients with unusual plan configurations, non-standard HCPCS coverage restrictions, or mid-year plan changes that have not yet propagated into the clearinghouse 271 response, manual verification through the plan’s provider portal or provider services line may provide more current and complete benefit information than the automated 271 response.
This does not make manual verification the preferred default it means having a clear exception workflow for MA patients whose automated eligibility results return incomplete or flagged data, routing those specific cases to a manual follow-up queue rather than relying on the automated result alone.
How Do You Implement Real-Time Eligibility Verification for DME?
Implementing real-time eligibility verification requires clearinghouse enrollment, platform API configuration, and a defined exception workflow for results that the automated system cannot resolve. The implementation is typically 4 to 8 weeks from start to full deployment.
What Prerequisites Are Required?
- Clearinghouse enrollment for 270/271 EDI: Active enrollment with at least one of Availity, Waystar, or Change Healthcare is required. 270/271 enrollment is separate from claim submission enrollment and requires its own setup with the clearinghouse and payer EDI departments. If your operation currently does manual eligibility checks without 270/271 enrollment, this is the first prerequisite to address.
- Core platform API access: The eligibility agent reads patient and order data from Brightree or NikoHealth and writes eligibility results back to the patient record via API. Confirm API access is enabled and that the relevant patient demographics and insurance fields are accessible via the API before implementation planning begins.
- NPI and taxonomy codes on file: The 270 transaction must include the rendering and billing provider NPI and taxonomy code. These must match the NPI Registry and the provider’s payer enrollment records. Mismatches between the NPI in the 270 transaction and the payer’s credentialing records return eligibility errors rather than benefit responses.
- HIPAA-compliant data handling: The eligibility agent handles PHI at every step. A signed Business Associate Agreement (BAA) with the clearinghouse and the eligibility platform vendor, SOC 2 Type II certification, and US-only data residency are required before any patient data touches the automated eligibility system.
- Exception queue workflow: Real-time eligibility handles the majority of standard eligibility queries without error. Exceptions for payer EDI timeouts, MA patients requiring manual portal verification, and COB scenarios requiring manual resolution must route to a defined queue with assigned staff and SLA. A real-time eligibility system without an exception workflow creates a gap where flagged orders sit without action.
What Does the Implementation Timeline Look Like?
- Week 1 (Clearinghouse audit): Confirm current 270/271 enrollment status with your clearinghouse. If enrollment is not current, initiate enrollment for Medicare, your top five Medicaid payers by volume, and your top five commercial payers by volume.
- Week 2 (Platform API setup): Connect the eligibility agent to Brightree or NikoHealth via API. Map patient demographics, insurance fields, and HCPCS code from the intake record to the 270 transaction fields.
- Week 3 to 4 (Payer testing): Test 270/271 transactions against live payer EDI endpoints for your top 10 payers by volume. Validate that 271 responses are returning all eight required data elements and that the parsing logic is correctly mapping response fields to patient record fields.
- Week 4 to 5 (Exception queue setup): Configure the exception queue for MA patients, EDI timeout cases, and COB scenarios. Assign staff. Define the manual follow-up SLA for each exception type.
- Week 5 to 6 (Parallel run): Run automated eligibility alongside manual verification for two weeks. Compare results. Validate that automated responses match manual check results for a representative sample of orders across payer types.
- Week 6 to 8 (Full deployment): Retire manual verification for all payer types where automated results have been validated. Manual verification continues only for exception queue cases. Activate delivery-trigger re-verification for orders with lead times above 48 hours.
What Results Are DME Operators Seeing With Real-Time Eligibility Verification?
The benchmarks below combine published industry data with operator-reported outcomes from DME providers who transitioned from manual to real-time eligibility verification during 2024 and 2025. Results vary by payer mix and existing clearinghouse configuration.
1. Staff Hours Recovered
A DME operation processing 300 orders per month and spending 18 to 22 minutes per manual eligibility check recovers 90 to 110 staff hours monthly after moving to real-time verification. At a fully loaded billing coordinator cost of 22 to 28 dollars per hour, that is 1,980 to 3,080 dollars in staff cost recovered per month, approximately 24,000 to 37,000 dollars annually from a single workflow step. AAHomecare’s 2023 Operational Survey benchmarks are consistent with this range for mid-size DME operations.
2. Eligibility Error Denial Rate
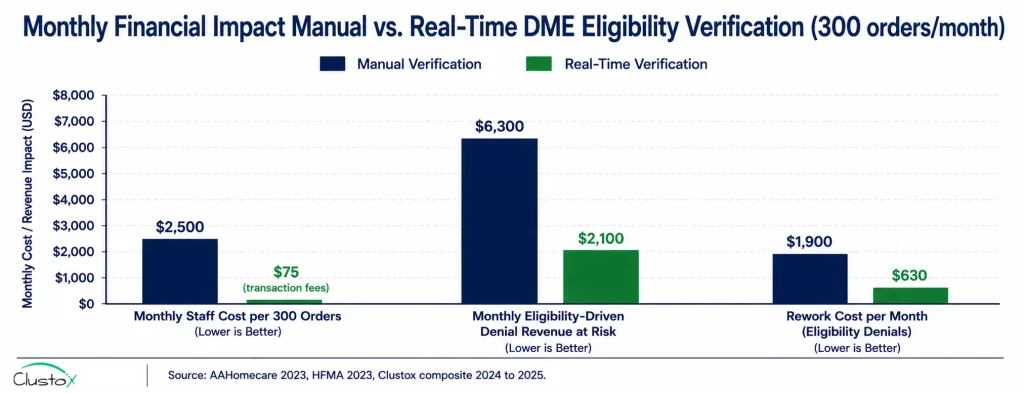
Eligibility-driven denials fall from 8 to 12 percent of claims to 2 to 4 percent of claims after full real-time eligibility implementation, per Clustox client composite data. At 300 claims per month and an average reimbursement of 350 dollars, reducing eligibility-driven denials by 6 percentage points recovers approximately 6,300 dollars per month in previously denied revenue before rework costs are applied. Combined with the 118 dollars per denied claim in rework cost reduction (HFMA), the total monthly financial benefit of real-time eligibility for a 300-order operation is approximately 8,000 to 12,000 dollars.
3. Intake-to-Fulfillment Time
Eligibility verification time falls from 18 to 22 minutes per order to under 60 seconds for standard payer types. Combined with other intake automation steps, DME operators using real-time eligibility as part of a full automated intake workflow report intake-to-fulfillment times under 4 hours for straight-through eligible referrals, compared to the 48 to 72-hour industry average for manual intake, per AAHomecare 2023.
4. Orders Processed Per FTE
DME operations using real-time eligibility and automated intake consistently report 200 to 280 orders processed per FTE per month, compared to the 80 to 110 per FTE baseline for manual intake operations. The same headcount handles more than twice the order volume, which means that revenue growth no longer requires a proportional increase in billing and intake staff.
What Are the Real Limits of Real-Time Eligibility Verification for DME?
Real-time eligibility verification significantly outperforms manual verification on speed, cost, and denial prevention for standard payer types. It has genuine limits that operators should understand before assuming full automation coverage.
- Not all payers support real-time 271 responses: Several smaller commercial payers and some state Medicaid programs return 271 responses in batch rather than real time, with turnaround times of 2 to 8 hours. For these payers, real-time verification is not available; the eligibility check returns the same day rather than in seconds. Confirm which of your top 10 payers by volume support real-time 271 responses before assuming real-time results across your full payer mix.
- Medicare Advantage plan-specific rules require additional configuration: As described in the MA section above, a standard 271 response from an MA plan confirms benefit category coverage but does not return plan-specific HCPCS coverage rules, PA thresholds, or documentation requirements. Operators with significant MA volume need an MA plan rules library alongside the automated eligibility check.
- Retro coverage changes are not caught automatically: If a patient’s coverage is terminated retroactively after a check has already passed, the automated system will not flag the change unless a second check is triggered. This is the primary remaining risk for real-time eligibility, and it is why delivery-trigger re-verification is an important operational safeguard for orders with longer lead times.
- HIPAA compliance requires documented vendor management: Every vendor in the automated eligibility workflow clearinghouse, eligibility platform, and data storage must have a signed BAA and current HIPAA compliance documentation. Adding a clearinghouse or eligibility API without updating the BAA register is a compliance gap that auditors consistently find during healthcare technology reviews.
Frequently Asked Questions
What Is the 270/271 EDI Transaction?
The 270 transaction is the ANSI X12 electronic eligibility inquiry submitted by a provider to a payer. It contains the patient's insurance member ID, the provider NPI, the date of service, and the service type code. The payer returns a 271 transaction the eligibility response with the patient's coverage status, benefit details, deductible and cost-sharing information, and any coverage restrictions or PA requirements. The 270/271 transaction set is the standard for electronic eligibility verification in the United States healthcare system. CMS publishes 270/271 implementation guides via the Medicare Learning Network for detailed technical specifications.
How Long Does Real-Time Eligibility Verification Take?
For payers that support real-time 271 responses, Medicare Part B administered through your MAC, major commercial payers, and many Medicare Advantage plans' automated eligibility verification returns results in under 60 seconds from submission of the 270 transaction. Payers that return batch 271 responses typically provide results within 2 to 8 hours. In both cases, the staff time required is near zero, compared to 18 to 22 minutes for manual phone verification.
Does Real-Time Eligibility Verification Work for Medicare Advantage?
Real-time 270/271 eligibility verification confirms MA enrollment and benefit category coverage for most MA plans. The limitation is that standard 271 responses do not return plan-specific HCPCS coverage rules, PA thresholds unique to the MA plan, or mid-year coverage policy changes that have not yet propagated into the EDI response. DME operators with significant MA patient volume need an MA plan rules library maintained alongside the automated check, updated quarterly at a minimum, to catch plan-specific coverage restrictions that standard EDI responses miss. CMS Medicare Advantage plan resources provide plan directories and summaries of benefits documents for each MA plan.
What Clearinghouses Support DME Eligibility Verification?
The three primary clearinghouses that handle 270/271 routing for DME providers are Availity, Waystar, and Change Healthcare. Each clearinghouse has different payer connectivity coverage, and your top payers may route through different clearinghouses. Confirm payer-specific clearinghouse routing for your top 10 payers by volume before implementing automated eligibility. Some DME billing platforms, including Brightree and NikoHealth, have native connectivity to one or more of these clearinghouses built into the platform.
How Does Eligibility Verification Integrate With Brightree?
Eligibility verification integrates with Brightree via its published REST API. The eligibility agent reads the patient demographics and insurance data from the Brightree patient record, submits the 270 transaction, receives the 271 response, and writes the parsed eligibility fields back to the appropriate fields in the Brightree order record. Eligibility results are stored in the Brightree audit trail per order. Brightree also supports native clearinghouse connectivity through Waystar and Availity, which can be used as the 270/271 routing layer without a separate clearinghouse setup. Brightree platform resources cover integration documentation for third-party eligibility tools.
When Does Manual Eligibility Verification Still Make Sense?
Manual verification through a payer portal or phone call remains appropriate in three scenarios. First, for MA patients whose automated 271 response returns incomplete or flagged data that cannot be resolved from the standard EDI response. Second, for payers that do not support 270/271 EDI at all, which is uncommon among major payers but can occur for small regional plans or workers' compensation payers. Third, for eligibility disputes where the automated result conflicts with what the patient or physician believes is covered, and the discrepancy needs to be resolved directly with the payer. In all three cases, manual verification should be a defined exception workflow rather than the default method.
What Is the ROI of Switching to Real-Time Eligibility Verification?
For a DME operation processing 300 orders per month and currently running manual phone eligibility, the financial case for real-time verification is straightforward. Staff cost savings from eliminating 18 to 22 minutes per check: approximately 2,000 to 3,000 dollars per month. Revenue recovered from reducing eligibility-driven denials from 8 to 12 percent to 2 to 4 percent of claims: approximately 4,000 to 6,300 dollars per month at 350 dollars average reimbursement. Rework cost reduction at 118 dollars per eliminated denied claim: approximately 1,200 to 1,900 dollars per month. Total monthly benefit: 7,200 to 11,200 dollars. Clearinghouse transaction costs at 0.25 dollars per check: approximately 75 dollars per month. Implementation is typically cost-positive within 30 to 60 days of full deployment. AAHomecare's 2023 Operational Survey provides payer-mix-adjusted ROI benchmarks for operations at different scale points.
Final Thoughts
The difference between manual and real-time eligibility verification is no longer just about speed. It is about operational accuracy, denial prevention, and whether your intake workflow can scale without adding headcount every time order volume grows.
Manual verification still creates the same recurring problems across DME operations: long hold times, incomplete HCPCS-level benefit details, missed prior authorization requirements, transcription mistakes, and eligibility data that becomes outdated before delivery. Real-time 270/271 verification removes most of those failure points by returning structured eligibility data directly into Brightree or NikoHealth in seconds instead of minutes.
The technology is not perfect, especially for complex Medicare Advantage edge cases and payer-specific coverage rules that still require human review. But for most DME providers, the operational and financial case is already clear.
Faster intake, lower eligibility-driven denial rates, reduced rework cost, and more orders processed per FTE make real-time verification one of the highest-ROI automation upgrades available in the DME revenue cycle today.