Skepticism about AI in DME billing is not ignorance. It is pattern recognition. Most operators have watched a software vendor promise workflow transformation and deliver a system that required more clicks, not fewer. That history is real, and it is a reasonable basis for caution.
Agentic AI in 2026 is different from the rules-based tools that failed before. It is also different from the AI that is genuinely not ready yet. This article draws that line clearly. The skeptic deserves an honest account, not a sales deck.
The evidence for AI in specific DME workflows, prior authorization, eligibility verification, and denial management, is strong enough to act on. The evidence for AI in other areas is thinner. This guide maps both. If you want the full architecture reference, the Agentic AI for DME pillar guide covers the complete stack. This article is for operators who are not there yet.
What This Article Covers
- Six objections skeptical DME operators raise, answered with evidence
- What Agentic AI actually does in DME billing and what it does not do
- Where the evidence is strong enough to act on and where it is not yet
- A readiness self-assessment to determine whether your operation is ready to start
- How to evaluate AI vendors without being misled by demos on synthetic data
- A phased starting plan that does not require betting the operation on one decision
Six Objections Skeptical DME Operators Raise, Answered Honestly
These are the real objections. Not strawmen. These are the questions that come up in every DME operator conversation before a decision to move forward or walk away.
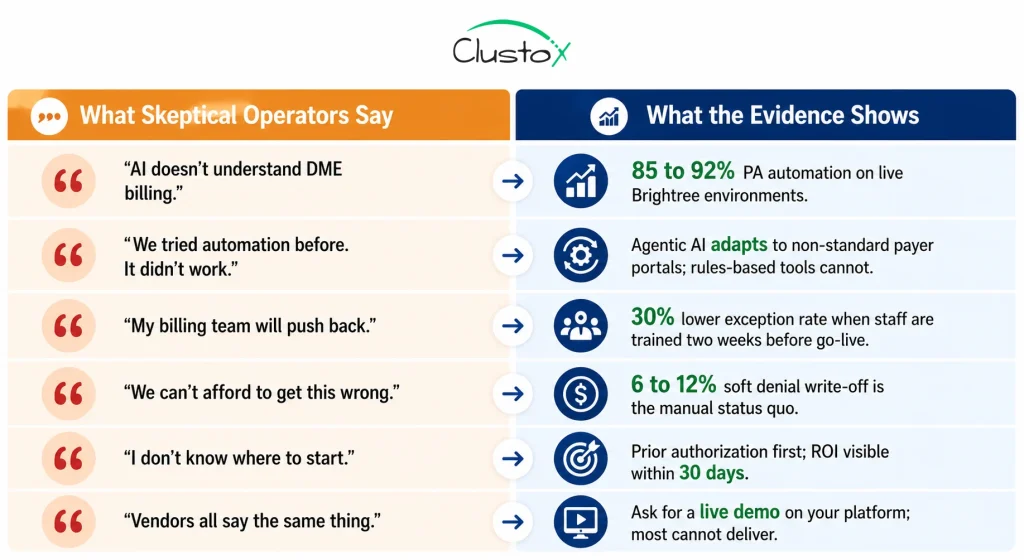
| What Skeptical Operators Say | What Is Actually True | What the Evidence Shows |
|---|---|---|
| "AI doesn't understand DME billing." | It does not need to understand it the way a human does. It needs to follow the rules reliably, every time, without forgetting. CMS LCD criteria do not require intuition. They require consistency. | Prior auth agents on Brightree and NikoHealth currently automate 85 to 92% of routine PA submissions with error rates below manual baselines. Per Clustox implementation data. |
| "We tried automation before. It didn't work." | Rules-based tools from five years ago are not the same as goal-directed Agentic AI. Rules-based tools fail when payer portals change. Agentic AI adapts. The two are structurally different. | Agentic AI workflows handle non-standard payer responses that rules-based tools cannot. The gap in capability is meaningful, not marketing. |
| "My billing team will push back." | They push back because the last technology change added work without reducing it. AI reduces their workload on routine orders. They spend time on exceptions that need judgment, not on data entry. | Operations that train billing staff two weeks before go-live see 30% lower exception rates in the first 30 days compared to those that train on the day of cutover. Per Clustox implementation data. |
| "We can't afford to get this wrong." | You can't afford to keep getting it wrong manually either. 6 to 12% of submitted DME claims are written off as unrecoverable. That is not a technology risk. That is the status quo. | A 48-hour AI Readiness Audit costs less than one recovered soft denial for most operations. It maps your risk before you commit to any implementation spend. |
| "I don't know which workflow to start with." | Prior authorization. It is the highest-volume, highest-friction workflow in every DME operation. The ROI is measurable within the first billing cycle. Everything else follows. | Prior auth automation typically reaches go-live in 8 to 12 weeks on Brightree or NikoHealth. Results are visible within 30 days of deployment. |
| "The vendors all say the same thing." | They do not all say the same thing when you ask them to demonstrate a complete PA cycle, from order creation to payer approval, with no human touchpoints, on your platform. Most cannot. | Ask for a live demo on Brightree or NikoHealth. If they demo a sandbox environment with synthetic data, that is your answer. |
What Is Agentic AI in DME Operations and How Is It Different From Traditional Automation?
Most operators have heard ‘AI’ used to describe everything from a simple autocomplete to a fully autonomous billing system. The term is doing too much work.
Agentic AI is goal-directed. You give it an objective, say ‘get this prior authorization approved,’ and it pursues that objective through multiple steps without needing a human to approve each one. It navigates payer portals, handles non-standard responses, and escalates only genuine exceptions.
This is different from rules-based automation, which executes a fixed script. If a payer portal changes its interface, a rules-based tool breaks. An Agentic AI agent adapts. It is also different from a chatbot or a copilot suggestion tool. For the technical architecture, see the DME AI stack guide. For this article, the operational definition is what matters.
Table of Contents
The Simple Test
Ask any AI vendor to demonstrate a complete prior authorization cycle. Start with an order in Brightree or NikoHealth. End with a payer approval number written back to the order record. No human touchpoints. On your platform, not a sandbox.
If they cannot do that, they are not selling what they say they are selling.
What Agentic AI Does and Does Not Do in DME OperationsAsk
This is the section most vendor pitches skip. Both columns matter.
| What Agentic AI Does in DME Operations | What Agentic AI Does Not Do |
|---|---|
| Submits prior authorization requests via payer portals, monitors status, and escalates stalled PAs to a human reviewer | Replaces clinical judgment on complex CRT documentation (K0800–K0899 requires a human specialist in the loop) |
| Runs real-time 270/271 eligibility checks at intake, PA submission, and claim drop without staff intervention | Conduct peer-to-peer clinical reviews when a payer requests one after a PA denial |
| Classifies incoming denials by root cause and drafts appeals with supporting documentation | Makes substantive decisions in response to RAC or TPE audit demand letters (AI assembles the package; humans decide) |
| Contacts CPAP patients via voice and SMS for re-supply outreach and pushes confirmed orders back to the platform | Fix a clinically inadequate LMN written by a referring physician |
| Tracks oxygen recertification schedules and alerts referring physicians 30 and 14 days before each deadline | Handles every MeOperationsportal at launch (10 to 20% of payer mix may require manual fallback initially) |
| Checks LMN completeness, ICD-10 to HCPCS alignment, and HCPCS modifier requirements before a claim drops | Guarantee claim approval; it maximizes the quality and speed of submission, not the payer's decision |
| Writes PA numbers, authorization status, and appeal outcomes back to order records in Brightree or NikoHealth | Operate without clean data in your Brightree or NikoHealth instance |
| Maintains a timestamped, attributable audit log of every automated action for TPE and RAC defense | Replace your billing team; it changes what they do, not whether you need them |
Where Is Agentic AI Still Limited in DME Operations?
Not every AI claim in DME is equally supported by evidence. These three workflows have the strongest track record in production environments.
1. Prior Authorization: The Clearest Case
Prior authorization is the workflow with the most evidence behind it. The HFMA 2024 Revenue Cycle Benchmarking Report documents a 6- to 9-day turnaround for manual PA processing. Agentic AI workflows on Brightree and NikoHealth consistently bring this below 48 hours for standard HCPCS categories.
The mechanism is clear. The agent pulls the order and LMN, checks documentation against the applicable CMS LCD criteria, submits via the payer portal, and monitors for status. It does not require clinical judgment on routine cases.
PA automation rate of 85 to 92% on routine submissions is consistent across Clustox implementations. The remaining 10 to 15% are escalated to a human reviewer with context assembled.
2. Eligibility Verification: Prevention Is Cheaper Than Recovery
Single-point eligibility checks at intake miss mid-year plan changes, benefit exhaustions, and coordination-of-benefits shifts. The OIG 2023 DME billing compliance report identifies documentation and eligibility errors as leading drivers of improper payments.
AI eligibility agents run 270/271 checks at intake, at PA submission, and at claim drop. They flag benefit-limit proximity and coordination-of-benefits issues before the claim goes out wrong.
Eligibility-driven soft denials drop 15 to 22% within 90 days of deployment. That is revenue not lost rather than revenue recovered. Prevention is cheaper.
3. Denial Management: Recovering What Was Being Written Off
The average DME provider writes off 6 to 12% of submitted claims, per the OIG 2023 DME billing compliance report. Most are soft denials: correctable errors that could be appealed but are not, because the billing team does not have time.
AI denial management classifies every denial by root cause and drafts the appropriate appeal automatically. It also feeds patterns upstream to prevent the same error on future claims.
18 to 27% of previously written-off soft denials are recovered within 90 days. Per Clustox implementation data across Brightree and NikoHealth clients.
What Results Are DME Providers Seeing From Agentic AI Today?
These metrics are from Clustox implementations on Brightree and NikoHealth, validated against HFMA 2024 and OIG 2023 benchmarks. Results vary by payer mix, order volume, and workflow maturity.
| Metric | Manual Baseline | With AI Automation | Source |
|---|---|---|---|
| Prior auth turnaround | 6–9 days per order (manual) | Under 48 hours | HFMA 2024; Clustox data |
| PA automation rate | 0% (fully manual) | 85–92% of routine PAs | Clustox implementation data |
| Soft denial write-off | 6–12% of submitted claims | 18–27% recovered in 90 days | OIG 2023; Clustox data |
| Eligibility denial rate | Single-check baseline | Down 15–22% | Clustox implementation data |
| Patient intake time | 45–60 min per new patient | 8–12 min (AI-assisted) | Clustox implementation data |
| CPAP re-supply patient reach | 30–40% (phone only) | 65–75% (voice + SMS) | Clustox implementation data |
| Orders per billing FTE/month | 80–120 complex orders | 200–240 orders | Clustox implementation data |
| Overall admin overhead | Baseline | 47% reduction at full deployment | Clustox implementation data |
Where Is Agentic AI Still Limited in DME Operations?
Honest accounting requires this section. Not everything that gets marketed as DME AI is performing equally well.
1. Complex Rehab Technology (CRT) Prior Authorization
For K0800 through K0899 categories (custom power wheelchairs, complex seating), documentation requirements are individualized and payer-specific.
AI assists with documentation completeness checks and submission logistics. The clinical coverage determination still requires a trained specialist. Do not attempt to fully automate CRT prior authorization without a human clinical reviewer.
2. Non-Standard Medicare Advantage Portals
AI agents work most reliably on payer portals with consistent interfaces. Some regional Medicare Advantage plans use non-standard portals that require a manual fallback at initial deployment.
Expect 10 to 20% of your payer mix to need manual fallback at go-live. This proportion declines as the agent learns each portal over the first 60 to 90 days.
3. Patient-Facing Conversations Beyond Structured Outreach
AI voice agents handle structured outreach well: CPAP resupply: Ask for confirmation, appointment reminders, and recertification scheduling. They do not handle nuanced patient conversations about coverage disputes or clinical questions.
The boundary is structured vs. unstructured. Within structured scripts on verified patient populations, AI voice outreach is production-ready. Outside that boundary, it is not.
4. AI Products That Cannot Demonstrate Live Results
The DME AI vendor space includes many products that are closer to rules-based tools with AI marketing. The test is a live demonstration.
If a vendor demos on synthetic data, demos in a sandbox environment, or cannot show a PA cycle from order to payer approval with no human touchpoints on Brightree or NikoHealth, they are not selling what they say they are.
Readiness Self-Assessment: Is Your Operation Ready to Start?
Use this before any vendor conversation. These are the variables that determine whether your implementation goes live on schedule or stalls for six months.
| Readiness Check | If Yes | If No / Unclear |
|---|---|---|
| Your DME platform is Brightree or NikoHealth | Ready to integrate | Legacy platform (TIMS, Bonafide): assess migration first |
| You have API access confirmed with your platform | Integration can begin | No API access: resolve before committing to any timeline |
| Your patient and order data quality is clean | AI will be accurate | Dirty data: expect higher exception rates at launch |
| Your top 10 payers are confirmed by the vendor | Full automation on major payers | Payer gaps: agree on manual fallback paths before go-live |
| You have a HIPAA BAA with your infrastructure provider | Compliant to process PHI | No BAA: this must be in place before PHI touches the AI layer |
| Your billing team knows what is changing before go-live | Smooth transition | No prep: expect a 30% higher exception rate in week one |
| You have documented your baseline metrics | ROI is measurable | No baseline: you cannot prove or disprove the result |
| You know which workflow to automate first | Ready to start | No priority: start with prior authorization, every time |
How Can DME Providers Evaluate AI Vendors Without Falling for Marketing Hype?
The DME AI vendor landscape is still early and highly uneven. Some vendors offer purpose-built healthcare automation platforms, while others simply repackage generic AI tools without understanding DME workflows, payer requirements, or compliance obligations.
Before committing to any automation project, operators should evaluate vendors against a set of practical, measurable criteria. The questions below often reveal the difference between a solution that can succeed in production and one that only performs well in a sales demo.
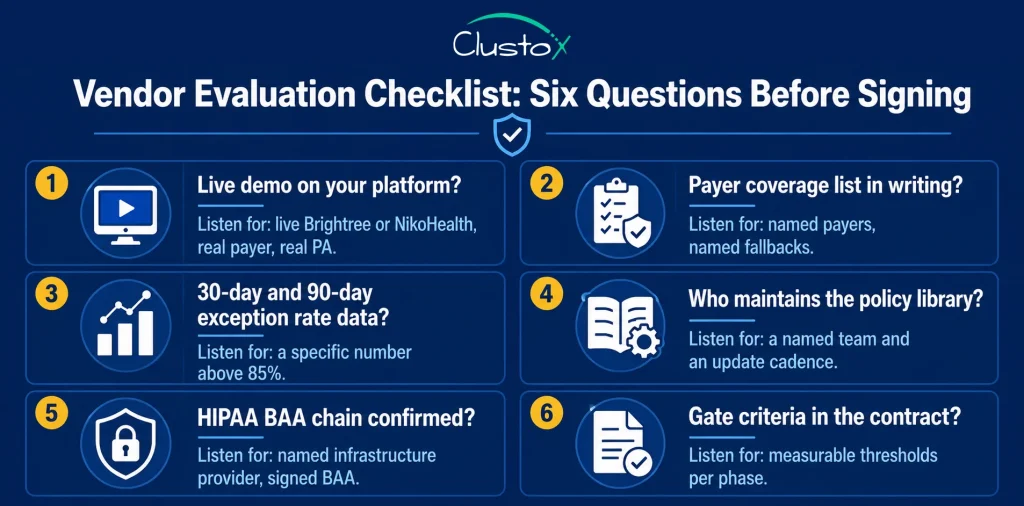
When reviewing vendor responses, focus on evidence rather than promises. Ask for live demonstrations, customer references, payer coverage documentation, HIPAA compliance records, and measurable performance benchmarks. Vendors that cannot provide these details typically struggle when deployments move from controlled demonstrations to real-world operations.
Once you’ve identified a vendor that meets these requirements, the next question becomes how to begin automation without introducing unnecessary operational risk.
What Is the Safest Way to Start Using Agentic AI in a DME Operation?
You do not need to commit to a full multi-workflow AI deployment on day one. The most successful DME automation projects start with a focused workflow, establish measurable results, and expand only after proving value.
A phased approach reduces implementation risk, shortens the path to ROI, and allows billing teams to adapt gradually while maintaining operational continuity.
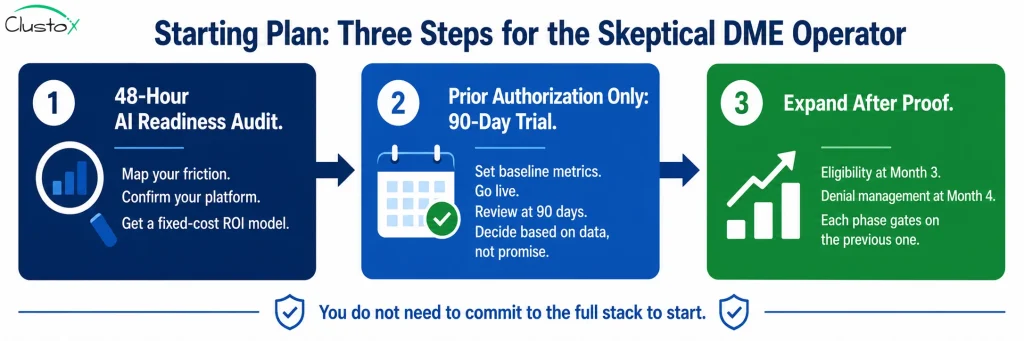
Step 1: The AI Readiness Audit
An AI Readiness Audit maps your current workflow friction, confirms your platform’s API integration feasibility, and produces a prioritized workflow plan with a fixed-cost ROI model. It costs less than most billing errors you are writing off this month.
It is also the only way to get a specific, honest answer to the question: which workflow should I automate first, and what will it cost?
Step 2: Prior Authorization Only, on a 90-Day Trial Logic
Commit to the prior authorization workflow only. Not eligibility. Not denial management. Just prior auth.
Set your baseline metrics before going live: current PA turnaround time and current orders per billing FTE per month. At 90 days, compare. If the PA automation rate is above 85% and turnaround is under 48 hours, the model is working.
If it is not working at 90 days, you have not built a six-workflow dependency. You have learned something specific about your operation that a good vendor will help you fix.
Step 3: Expand Only After Proof
Add eligibility verification at Month 3. Add denial management at Month 4. The sequence matters. See the full phased roadmap in the DME AI stack guide for the complete phase-by-phase plan with gate criteria.
Each phase builds on a foundation that the previous phase established. Skipping phases creates failure modes that look like AI problems but are actually sequencing problems.
Still On The Fence? Talk To Someone Who Has Done This.
Our AI Readiness Audit maps exactly which workflows are costing you the most, which automation delivers the fastest return, and what your implementation roadmap looks like.
Frequently Asked Questions
What is the difference between Agentic AI and the automation tools we tried before?
Rules-based automation executes a fixed script. If a payer portal changes its interface, or a payer sends a non-standard response, the tool breaks, and a human has to fix it. Agentic AI is goal-directed. It pursues an outcome through whatever steps the payer requires, adapts to non-standard responses within defined parameters, and escalates only genuine exceptions to a human. The structural difference is meaningful. It is not a marketing distinction.
What happens to our billing team if we automate prior auth and eligibility?
They shift from processing every order to reviewing exceptions. Instead of manually building PA submissions, they review the 10 to 15% of cases the AI cannot complete without human judgment: peer-to-peer escalations, documentation gaps, and non-standard payer responses. Operations that brief and train billing staff two weeks before go-live consistently see lower exception rates and smoother transitions than those that announce the change on the day it happens.
We are on TIMS, not Brightree or NikoHealth. Can we still use Agentic AI workflows?
The honest answer is that TIMS has limited API access, which significantly increases AI integration complexity and cost. In most cases, the cost of AI integration on TIMS exceeds the cost of migrating to NikoHealth and then implementing the AI layer. A 48-hour AI Readiness Audit will give you a specific cost comparison for your situation before you commit to either path.
How do I know if a DME AI vendor is selling what they say they are selling?
Ask for a live demonstration on your Brightree or NikoHealth environment. Not a sandbox, not synthetic data. A complete prior authorization cycle: from order creation to payer approval number written back to the order record, with no human touchpoints. If they cannot deliver that on your platform, the product is not what it claims to be. Also ask for the exception rate at 30 days and 90 days. If they cannot give you a specific number, they have not measured their own results.
What does a 48-hour AI Readiness Audit actually produce?
It maps your current workflow friction across the six core DME workflows: prior auth, eligibility, denial management, patient intake, re-supply outreach, and recertification. It confirms your platform's API integration feasibility. It identifies the workflow to automate first and the workflow to automate second. It produces a phased implementation plan with a fixed-cost ROI model for each phase. The output is a specific, actionable plan for your operation, not a generic framework.
How long before we see results after going live with prior auth automation?
PA turnaround time improvement is visible within the first two to four weeks of go-live, as the agent begins processing routine submissions without manual intervention. Soft denial recovery from the denial management workflow shows up within the first billing cycle after that workflow is deployed, typically 90 days after the prior auth workflow stabilizes. CPAP re-supply order capture improvement appears in the first re-supply cycle after the voice and SMS agent is deployed.
What is the risk if we implement AI and it does not work as expected?
If you follow the phased approach, the risk is bounded. If the prior authorization automation does not reach an 85% automation rate with an error rate below your manual baseline within 90 days, you have not committed to five more workflows built on top of it. You have one workflow underperforming, with specific data about why. A good implementation partner will diagnose and fix it. The risk of not automating is also real: 6 to 12% of your submitted claims are currently being written off as unrecoverable soft denials. That is not a future risk. That is happening now.
Is Agentic AI for DME billing HIPAA compliant?
A properly architected system is HIPAA compliant, but compliance is an architecture requirement, not a product feature. All AI processing of Protected Health Information must occur under signed HIPAA Business Associate Agreements with each infrastructure component: the DME platform, the AI inference provider (AWS Bedrock, Azure OpenAI, or GCP Vertex AI), and any voice or SMS platform used for patient outreach. Ask every vendor for the BAA chain before any PHI flows into the system.
What is the realistic cost of getting started with AI in our DME operation?
The 48-hour AI Readiness Audit is the right first cost: it is a fixed price, it maps your specific operation, and it produces an ROI model before you commit to any implementation spend. Implementation costs for prior auth and eligibility automation on Brightree or NikoHealth vary by operation size, payer mix, and data quality. A well-scoped implementation produces measurable ROI within the first billing cycle after go-live, typically 30 to 60 days, through recovered soft denials and PA turnaround improvement alone.
Conclusion
Your skepticism has served you well. It has helped you avoid technology investments that promised transformation but delivered more complexity, more manual work, and little measurable return. That same skepticism should also encourage a hard look at whether maintaining the status quo is becoming the more expensive option.
The evidence for Agentic AI in prior authorization, eligibility verification, and denial management is now strong enough for DME providers to evaluate seriously. The most effective approach is not a full-scale transformation overnight. It is starting with a single workflow, measuring results, and expanding only when the data supports the next step.
The operators who have taken that first step are processing significantly higher order volumes with the same billing teams, reducing administrative burden, and improving turnaround times.
Meanwhile, organizations that continue relying entirely on manual workflows face increasing reimbursement pressure, staffing challenges, and preventable revenue leakage from avoidable denials.
Agentic AI is not a replacement for experienced DME professionals. It is a tool for removing repetitive administrative work so teams can focus on the exceptions, decisions, and patient interactions that require human expertise.
The question is no longer whether AI will become part of DME operations. The question is which workflows make sense to automate first. As adoption expands, many providers are moving beyond individual automation projects toward a broader DME Operations AI Stack, where intake, eligibility verification, prior authorization, documentation, denial management, and patient outreach work as connected workflows rather than isolated processes.