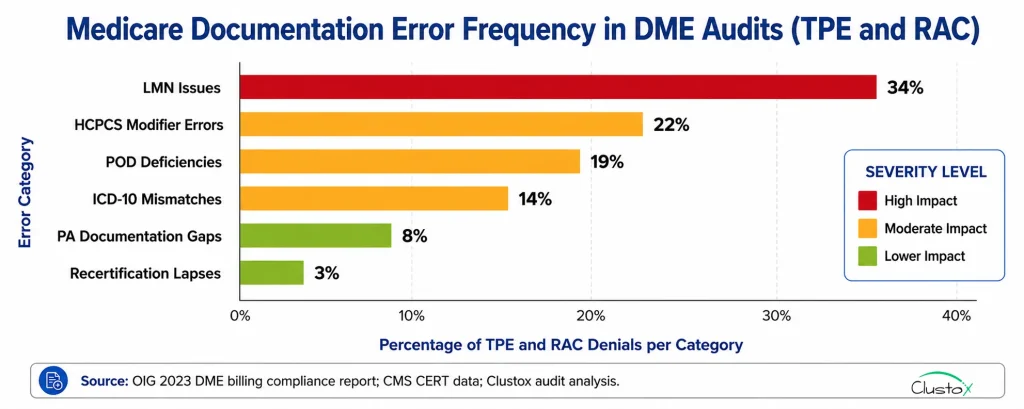
Medicare documentation errors are the primary driver of DME claim denials and audit recoupments. They are not rare edge cases. The OIG’s 2023 DME billing compliance report found documentation deficiencies account for the majority of improper payments.
CMS TPE audits specifically target HCPCS categories with known error patterns. If you bill high volumes of E0601 (CPAP), E1390 (oxygen concentrators), or K0800-series power wheelchairs, your categories receive the most scrutiny.
This article gives you two things: a clear map of the ten most common errors and the audit programs that find them, and a 41-item checklist across six categories that your billing team can use on every order. An AI documentation agent can run this checklist automatically in Brightree or NikoHealth; this article is the human-readable version of that logic.
What This Article Covers
- The ten most common Medicare documentation errors in DME and which audit programs catch each one
- How TPE, RAC, ZPIC, and UPIC audits work and what they target in DME billing
- A 41-item printable audit-proof checklist across six documentation categories
- How AI documentation workflows on Brightree and NikoHealth prevent errors before claims drop
- What to do when an audit notification arrives, and documentation is incomplete
How Do Medicare Audits Work for DME Providers?
Four distinct programs audit DME billing. Each has different triggers, contractors, and response requirements. Knowing which one is contacting you determines how to respond.
| Audit Type | Contractor | Focus Area | Sample Size | Response Window |
|---|---|---|---|---|
| TPE (Targeted Probe and Educate) | Medicare Administrative Contractors (MACs) | High-error HCPCS categories; provider billing patterns | 20–40 claims per round | 45 days from request |
| RAC (Recovery Audit Contractor) | CMS-contracted firms (Cotiviti, Performant) | Overpayments; high-value categories; pattern-based selection | Varies; large samples possible | 45–60 days from demand |
| ZPIC | Absorbed into UPIC program (2019) | Fraud, waste, and abuse; statistical outlier billing | Targeted; often provider-wide | Varies; payment suspension possible |
| UPIC (Unified Program Integrity) | Health Integrity, Qlarant, Safeguard Services | Fraud, waste, and abuse across Medicare and Medicaid | Targeted; can be broad | 15–30 days; extensions possible |
TPE audits are the most common first contact. A MAC selects a sample of 20 to 40 claims, reviews documentation, and provides feedback. Providers with high error rates enter additional rounds. The CMS TPE process is documented at CMS.gov.
RAC audits focus on recovering overpayments. RAC contractors are paid a contingency fee on recovered funds. DME is a consistent RAC target. Power wheelchairs, oxygen equipment, and CPAP supplies have all been RAC focus categories. See OIG Medicare program integrity reports for current focus areas.
Key Audit Benchmarks
DME improper payment rate: elevated in CMS FY2023 CERT report; documentation deficiencies are the primary driver, per CMS.gov/CERT.
Table of Contents
Soft denial write-off rate: 6 to 12 percent of submitted DME claims, per OIG 2023 DME billing compliance report.
TPE response window: 45 days from MAC record request; records not submitted are treated as missing.
RAC demand letter response: 45 to 60 days to file a rebuttal or appeal with the QIC.
The Ten Most Common Medicare Documentation Errors in DME
The table below maps each error to the HCPCS categories most affected, the audit type most likely to identify it, and the consequence for the provider. These are the errors appearing most frequently in CMS TPE feedback letters and OIG audit findings.
| # | Documentation Error | HCPCS / Category Affected | Audit Type | Consequence |
|---|---|---|---|---|
| 1 | Missing or incomplete Letter of Medical Necessity (LMN) | All PA-required categories: E0601, E1390, K0001–K0108 | TPE, RAC | Prior auth denial; claim recoupment |
| 2 | LMN not signed by ordering physician or NP/PA | All LMN-required categories | TPE, RAC, ZPIC | Claim void; overpayment demand |
| 3 | LMN date predates or exceeds validity window | E1390, E0601, custom mobility | TPE, RAC | Claim denial; requires re-documentation |
| 4 | Missing face-to-face examination documentation | K0800–K0899 (power wheelchairs), CRT | TPE, RAC | Full claim denial; high recoupment risk |
| 5 | ICD-10 code does not support HCPCS medical necessity | All categories; O2, CPAP, mobility especially | RAC, ZPIC | Medical necessity denial; appeal required |
| 6 | Incorrect or missing HCPCS modifier (KX, GA, GZ) | E0601, E1390, A9270, L codes | RAC, TPE | Claim rejection or underpayment |
| 7 | Prior authorization number missing on claim | All PA-required categories under CMS PA program | Payer edit | Automatic denial; resubmission delay |
| 8 | Proof of delivery (POD) documentation incomplete | All equipment; CPAP supplies especially | TPE, RAC | Claim denial; overpayment demand |
| 9 | Oxygen recertification not completed within CMS window | E1390, E0431, E0434 | TPE, UPIC | Retroactive denial; audit exposure |
| 10 | Advance Beneficiary Notice (ABN) not obtained or filed | Non-covered or Medicare-excluded items | ZPIC, UPIC | Liability shifts to provider; fraud risk |
Deep Dive: The Five Errors That Create the Most Audit Exposure
The 5 errors below create the most audit exposure. They affect the largest HCPCS categories, carry the highest recoupment dollar value, or signal a systemic documentation problem to the auditing contractor.
Error 1: Missing or Incomplete Letter of Medical Necessity
The LMN is the foundation of every DME claim. Without a complete, current, signed LMN, no other documentation saves the claim in a TPE or RAC review.
The most common failure is not a missing document. It is an LMN with a generic necessity statement that lacks the diagnosis code linkage, clinical findings, and equipment specification that CMS LCD requirements mandate.
For CPAP (E0601), the LMN must reference a qualifying sleep study with an AHI of 15 or greater. For oxygen (E1390), it must reference a qualifying SpO₂ or ABG result at or below 88% on room air.
Error 2: ICD-10 Code Does Not Support HCPCS Medical Necessity
RAC contractors use automated edits to flag ICD-10 to HCPCS mismatches before a human reviewer sees the claim. This is a fast, low-effort denial for the contractor.
Common examples: billing E1390 with a hypertension diagnosis rather than a qualifying respiratory code, or billing K0001 with a diagnosis that does not establish ambulatory limitation.
AI document intelligence agents trained on CMS LCD databases catch these mismatches before the claim drops. This is a RAG (Retrieval-Augmented Generation) application running on Brightree or NikoHealth.
Error 3: Incorrect or Missing HCPCS Modifier
The KX modifier certifies that all applicable LCD criteria are met and documented. Billing KX without complete documentation is a compliance violation, not just a coding error.
The most common pattern: KX applied to routine CPAP and oxygen claims without verifying that every LCD element is actually in the patient file.
An AI modifier validation check confirms, before KX is applied, that the qualifying test result, signed LMN, physician credentials, and equipment specification are all present. If any element is missing, KX is blocked, and the order is flagged.
Error 4: Incomplete Proof of Delivery
Proof-of-delivery failures are a high-volume RAC audit finding. The most common failure is not a missing document. It is a POD in which the patient’s name is printed, but the signature is absent, or in which the delivered item description is generic.
A POD that says ‘medical equipment delivered’ does not satisfy the documentation requirement for an E0601 CPAP device. The POD must identify the device specifically.
Digital POD workflows with electronic signature capture, integrated with Brightree or NikoHealth, eliminate this problem. The item description on the POD pulls from the order record, ensuring HCPCS-level specificity.
Error 5: Lapsed Oxygen Recertification
Oxygen recertification follows a defined CMS schedule: initial certification, 90-day recertification, and annual recertification. The applicable oxygen LCD governs each window.
Missing any point in that schedule means the subsequent claims lack current documentation support. This creates both denial risk and potential fraud exposure if the pattern is systematic.
This error is almost entirely preventable with automated tracking. Per Clustox implementation data, providers running automated recertification tracking see missed recertification rates drop below 1% within 90 days of deployment.
The Audit-Proof Documentation Checklist: 41 Items Across Six Categories
The checklist below covers six documentation categories. Use it per order. Run it against a sample of your last 30 days of claims to identify which categories have the most gaps.
Those gaps are your audit risk profile. They are also the workflows where AI automation delivers the fastest return.
| Documentation Requirement | Action / Verification Note | |
|---|---|---|
| Section 1: Letter of Medical Necessity (LMN) Requirements | ||
| □ | LMN is present for every PA-required order in the patient file | Required for E0601, E1390, K0001–K0899, L0650–L0651, and all custom equipment |
| □ | LMN is signed by the ordering physician, NP, or PA within scope of practice | Unsigned LMNs are the leading TPE failure point; electronic signatures are acceptable if platform-supported |
| □ | LMN signature date falls within the applicable validity window per CMS LCD | CPAP LMNs valid 1 year; oxygen LMNs require 90-day and annual recertification |
| □ | LMN includes the patient ICD-10 diagnosis code and a medical necessity statement tied to that diagnosis | Generic statements such as 'patient needs CPAP' are insufficient; diagnosis must link to necessity |
| □ | LMN specifies the exact HCPCS code and equipment description being ordered | Respiratory equipment' is not sufficient for E0601; the LMN must name the device |
| □ | LMN is accessible in the patient's medical record, not only in the billing file | Auditors request the medical record; both files must be consistent |
| □ | For CPAP (E0601): LMN includes sleep study results with AHI score meeting CMS coverage threshold | AHI of 15 or greater required for standard CPAP coverage per applicable LCD |
| □ | For oxygen (E1390): LMN includes qualifying SpO₂ or ABG test results meeting CMS threshold | SpO2 at or below 88% on room air, or equivalent ABG result, is required |
| Section 2: Face-to-Face Examination Documentation | ||
| □ | Face-to-face exam documentation is present for all K0800–K0899 and CRT orders | Required per CMS; exam must occur no more than 6 months before the order date |
| □ | Documentation includes the examining clinician's name, credentials, date of exam, and findings | Missing clinician credentials are a common TPE failure point for CRT categories |
| □ | Exam was conducted by the ordering physician or treating clinical staff | CMS requires the exam to be conducted by the ordering practitioner or their treating clinical staff |
| □ | For K0800–K0899: documentation includes mobility assessment and functional limitation findings | Must document why a less complex device cannot address the patient's mobility limitation |
| □ | Face-to-face notes are consistent with the LMN and order record | Inconsistencies between notes and LMN language are a primary audit red flag |
| Section 3: Prior Authorization Documentation | ||
| □ | Prior authorization obtained for all orders in CMS PA-required categories before delivery | PA-required categories listed at CMS.gov/Medicare/Prior-Authorization-Program |
| □ | PA number recorded in Brightree or NikoHealth and included on the claim (837, CLM05 field) | Missing PA number is an automatic denial; the AI prior auth agent should write it to the order record |
| □ | PA approval documentation retained in the patient file (payer letter or portal screenshot) | Digital copies in Brightree or NikoHealth are acceptable; original payer letter preferred |
| □ | PA request included all required clinical documentation (LMN, test results, face-to-face notes where applicable) | Incomplete PA documentation is the leading cause of PA denials; AI document check prevents this |
| □ | Equipment delivery date falls within the PA validity window | Delivering equipment after PA expiration is a recoupment risk even if the original PA was valid |
| □ | For denied PAs: peer-to-peer review was requested and documented within the payer window | Most payers allow 24 to 72 hours to request peer-to-peer; document request date and outcome |
| Section 4: Proof of Delivery (POD) Documentation | ||
| □ | Proof of delivery document is present for every delivered item | POD is required for all DME equipment and supplies; missing POD is a leading RAC finding |
| □ | POD includes patient or authorized representative signature and date | Unsigned POD is treated as no delivery; electronic signature is acceptable on supported platforms |
| □ | POD clearly identifies the delivered item including HCPCS code, description, and quantity | Vague descriptions such as 'medical supplies' are not sufficient |
| □ | POD date matches or precedes the claim service date | Claiming before confirmed delivery is a fraud risk and an automatic audit finding |
| □ | For CPAP supplies: POD includes serial or lot number for items requiring Medicare tracking | Required for certain CPAP equipment under Medicare HCPCS tracking requirements |
| □ | Delivery records are retained for a minimum of 7 years per Medicare record retention requirements | Medicare requires 7 years for billing records; use this window rather than the 6-year HIPAA minimum |
| □ | POD documentation is stored in Brightree or NikoHealth and retrievable within 45 days of a TPE request | TPE contractors allow 45 days; records not submitted within the window are treated as missing |
| Section 5: HCPCS Coding and Modifier Accuracy | ||
| □ | HCPCS code matches the equipment actually delivered, not a higher-priced substitute | Upcoding is a fraud and abuse risk; the billed code must match the delivered item exactly |
| □ | All required HCPCS modifiers are included on the claim (NU, RR, KX, GA, GZ as applicable) | Missing KX on CPAP and oxygen claims is a common denial cause; KX certifies medical necessity criteria are met |
| □ | KX modifier is used only when all applicable LCD criteria are fully documented and met | Using KX without complete documentation is a compliance violation and an audit trigger |
| □ | GZ modifier is applied for items expected to be denied as not medically necessary when no ABN is on file | GZ signals the item does not meet necessity criteria; incorrect use creates audit exposure |
| □ | GA modifier is applied only when an ABN has been obtained and is on file before service delivery | GA without an ABN on file is a compliance error; confirm ABN is in the patient record before billing |
| □ | ICD-10 diagnosis codes on the claim support the medical necessity of the billed HCPCS code | ICD-10 to HCPCS mismatches are a primary RAC audit selection criterion |
| □ | HCPCS codes are billed at the correct fee schedule rate for your MAC jurisdiction | Rates vary by jurisdiction; billing at the wrong rate creates over- or under-payment risk |
| Section 6: Recertification and Ongoing Compliance Documentation | ||
| □ | Oxygen recertification completed within the CMS-required window (90 days and annually per LCD criteria) | Missed windows cause retroactive claim denial; automate tracking in Brightree or NikoHealth |
| □ | Recertification LMN is signed by the ordering physician and includes current clinical findings | A recertification LMN from a different physician than the original order requires updated documentation |
| □ | Recertification includes updated SpO2 or ABG results meeting current CMS coverage thresholds | Previous qualifying results do not carry forward; thresholds must be re-met at each recertification |
| □ | CPAP compliance data (device usage reports) reviewed and retained at the 90-day mark | CMS requires CPAP compliance documentation at 90 days; non-compliant patients require reassessment |
| □ | Capped rental tracking is current and claims match the correct rental month (months 1–36 per CMS rules) | Billing beyond Month 13 for capped rental equipment without conversion to purchase is a fraud risk |
| □ | ABNs are issued and retained for all items that may not meet Medicare coverage criteria | ABN must be issued before providing the service; a post-service ABN has no legal effect |
| □ | All documentation is indexed and retrievable in Brightree or NikoHealth within the 45-day audit window | Disorganized records not retrieved in time are treated as missing during the audit |
| □ | AI audit trail log is active and capturing every automated action with timestamps | A complete AI audit log provides defensible documentation for every automated workflow action |
How AI Documentation Workflows Prevent These Errors on Brightree and NikoHealth
Every item on the checklist is a decision point that can be automated. This connects directly to the DME AI stack architecture covered in our separate guide.
Here is how automation maps to each category.
LMN Completeness Check
An AI document intelligence agent, built on an LLM with a RAG pipeline querying CMS LCD databases, checks every required LMN element before the order proceeds to PA submission.
Missing elements are flagged to the billing coordinator with a specific list of what is needed. For CPAP orders, it confirms the AHI score meets the coverage threshold. For oxygen, it confirms the SpO₂ or ABG result.
ICD-10 to HCPCS Validation
The agent queries the policy library for the applicable LCD and checks the billed ICD-10 against the covered diagnosis list for that HCPCS category.
Mismatches are flagged to the coding team before the claim is generated. This catches the ICD-10 errors that would otherwise produce an automatic RAC denial months after delivery.
HCPCS Modifier Gating
The KX modifier is blocked from the claim record until the agent confirms all KX qualification criteria are documented. GA is verified against ABN presence. NU and RR modifiers are validated against the order type.
Modifier errors that previously required a coding reviewer to catch are caught automatically before any human touches the claim.
PA Documentation Logging
The prior auth agent records the PA number directly to the order record in Brightree or NikoHealth at the moment of approval. PA approval documentation is attached automatically.
The claim generation process includes a PA number validation check. If no PA number is present for a PA-required HCPCS category, the claim does not drop until the number is added.
POD Tracking and Retrieval
Digital POD workflows with electronic signature capture, integrated with Brightree or NikoHealth, eliminate unsigned PODs.
The delivered item description pulls from the order record, ensuring HCPCS-level specificity. All POD records are indexed and retrievable by claim number, making TPE response a report pull rather than a records search.
Recertification Automation
The recertification agent tracks every active oxygen patient’s certification schedule and triggers physician outreach 30 and 14 days before each deadline.
Patients who do not recertify within the window are flagged before the next billing cycle, not after a denial arrives. This connects to the broader healthcare workflow automation framework covered in our separate article.
What to Do When a TPE or RAC Audit Notification Arrives?
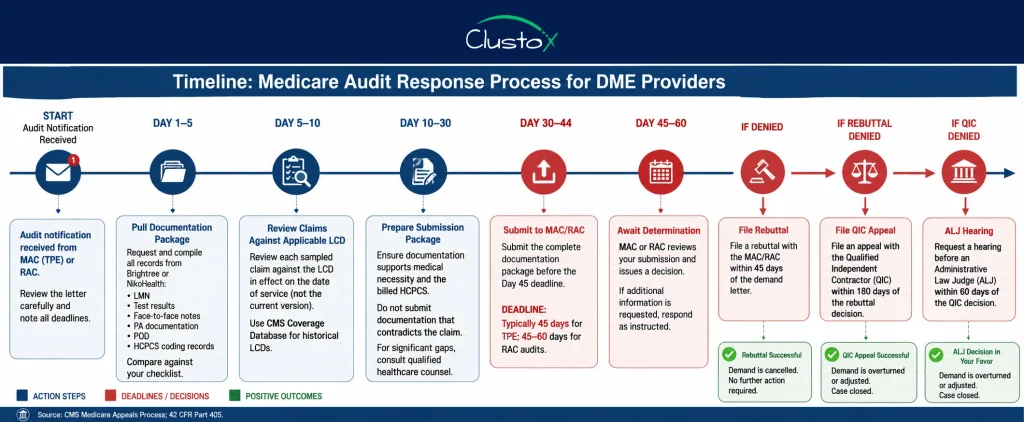
When a Targeted Probe and Educate (TPE) or Recovery Audit Contractor (RAC) audit notification is received, it is critical to respond promptly and accurately. Documentation for all sampled claims must be submitted within the required timeframe, typically 45 days for TPE audits and 45–60 days for RAC audits.
1. Gather Complete Documentation for Every Sampled Claim
Request and compile all relevant records from your documentation system (e.g., Brightree or NikoHealth), including:
- Letter of Medical Necessity (LMN)
- Test results
- Face-to-face encounter notes
- Prior authorization (PA) documentation
- Proof of Delivery (POD)
- HCPCS coding records
Before submission, compare all records against your internal audit checklist to ensure completeness and consistency.
2. Review Claims Against the Applicable LCD
Each sampled claim should be reviewed against the Local Coverage Determination (LCD) that applies to the billed HCPCS code category.
Important: Use the LCD version that was in effect on the date of service, not the current version. Historical LCD versions are available through the CMS Medicare Coverage Database.
3. Identify Documentation Deficiencies Before Submission
Carefully evaluate whether the LMN and supporting documentation adequately support the claim.
- Do not submit documentation that contradicts the claim.
- If the documentation contains significant gaps or does not support medical necessity, submitting it may effectively confirm the error.
- For claims with substantial deficiencies or potential liability, consult qualified healthcare legal counsel before responding.
4. Monitor TPE Error Rates
Under the TPE program, a high error rate can trigger additional audit rounds.
- If the Medicare Administrative Contractor (MAC) identifies errors in more than 20% of reviewed claims, a second review round is likely.
- Review the TPE feedback letter carefully and calculate your error rate.
- Use the findings to improve documentation and billing processes before the next review cycle.
5. Respond Promptly to RAC Demand Letters
If an RAC audit results in a demand letter:
- File a rebuttal within the specified rebuttal period, generally 45 days from the date of the demand letter.
- When the demand is incorrect, a successful rebuttal may eliminate the repayment demand without requiring a full administrative appeal.
6. Implement Corrective Actions After the Audit
Audit findings should be used to strengthen compliance procedures and reduce future risk.
Recommended actions include:
- Updating documentation and claim review checklists
- Revising workflow processes to address identified weaknesses
- Providing targeted training to billing and documentation staff
Training should focus specifically on the errors identified during the audit, as targeted education is generally more effective than broad, generic compliance training.
Is Your DME Documentation Audit-Ready?
We map your highest-risk documentation workflows, identify your top denial root causes, and build an automated checklist into your Brightree or NikoHealth environment.
Frequently Asked Questions
What does a TPE audit involve for a DME provider?
A TPE audit is conducted by a Medicare Administrative Contractor (MAC). The MAC selects 20 to 40 claims in a specific HCPCS category and requests supporting documentation. You have 45 days to respond. The MAC reviews documentation against the applicable LCD and provides a determination and feedback letter. Providers with high error rates enter additional review rounds. The full TPE process is described at CMS.gov.
What is the difference between a TPE audit and a RAC audit?
TPE audits are educational in intent. They identify errors and provide feedback, with escalating rounds for providers who do not improve. RAC audits focus on overpayment recovery. RAC contractors are paid a contingency fee on funds recovered, so they target high-value categories and systematic error patterns. RAC audits produce demand letters; TPE audits produce feedback letters. Both require the same documentation response discipline.
What happens if I receive an RAC demand letter?
You must either pay the demanded amount or file a rebuttal within 45 days. A successful rebuttal cancels the demand without requiring a full administrative appeal. If the rebuttal is denied, you can file a Redetermination request, then a QIC appeal, and then an ALJ hearing if needed. Each level has a specific filing window. Consult qualified healthcare counsel before responding to demand letters with significant dollar amounts.
Does a Letter of Medical Necessity expire?
Yes. LMN validity windows are defined by the applicable CMS Local Coverage Determination. CPAP device LMNs (E0601) are typically valid for one year. Oxygen LMNs require recertification at 90 days and annually. Power wheelchair LMNs have validity requirements tied to the face-to-face examination date. Using an expired LMN creates denial risk. Automated recertification tracking in Brightree or NikoHealth prevents this by alerting the referring physician before each deadline.
What does the KX modifier mean, and when should I use it?
The KX modifier certifies to Medicare that all applicable LCD criteria are met and documented in the patient's medical record. It is required on claims for CPAP (E0601), oxygen (E1390), and many other DME categories. Using KX when the documentation does not support it is a compliance violation. An AI HCPCS modifier validation check confirms all KX criteria are documented before the modifier is applied, preventing both the denial and the compliance risk.
How does AI prevent Medicare documentation errors in DME billing?
AI document intelligence agents, built on LLMs with RAG pipelines querying CMS LCD databases, check every required documentation element before a claim drops. The LMN completeness check confirms physician signature, diagnosis linkage, qualifying test results, and equipment specification. The ICD-10 to HCPCS validation confirms the diagnosis supports the billed category under the applicable LCD. The KX modifier gate blocks the modifier until all criteria are confirmed. The PA number check prevents claims from dropping without authorization. These checks run automatically on every order in Brightree or NikoHealth.
What records do I need to submit in a Medicare audit response?
For a TPE or RAC audit, you typically need: the signed and dated LMN; physician orders; qualifying test results referenced in the LMN (sleep study, SpO2, ABG); face-to-face examination notes where required; proof of delivery with patient signature; prior authorization documentation; and relevant medical record entries supporting necessity. For oxygen claims, recertification documentation for the relevant period is also required. Organize records by claim number and submit in the format specified by the contractor.
How long must DME providers retain Medicare billing documentation?
Medicare billing records must be retained for a minimum of seven years, per CMS billing documentation retention requirements. This is one year longer than the standard HIPAA minimum of six years. For Brightree and NikoHealth users, confirm that the platform's data retention policy meets or exceeds seven years. Paper records that cannot be produced within the 45-day TPE window are treated as missing.
Can the documentation checklist in this article be used for Medicare Advantage claims?
The core requirements for most HCPCS categories are similar between traditional Medicare and Medicare Advantage (Part C), but MA plans have authority to establish their own coverage criteria. Some MA plans impose stricter documentation requirements than traditional Medicare. Always verify the specific MA plan's coverage policy for the billed HCPCS category in addition to the applicable CMS LCD. The checklist in this article is based on CMS Medicare Part B standards and should be supplemented with plan-specific requirements for MA billing.
Conclusion
Medicare documentation errors in DME are preventable. Every error in the table of ten, and every item in the 41-item checklist, is a decision point in the order workflow that can be caught before the claim drops.
Run the checklist against a sample of your last 30 days of claims. The categories with the most unchecked boxes are your audit risk profile. They are also the workflows covered in our DME AI stack guide that deliver the fastest return when automated.
The 48-hour AI Readiness Audit maps your documentation risk, identifies your top error categories, and shows you which workflows to automate first. It is the right first step for any DME operation that has received a TPE feedback letter, is preparing for a RAC review, or simply wants to understand its documentation gaps before an auditor finds them.