
Switching HME software is not like changing a SaaS tool. It means migrating patient records, retraining billing staff, remapping payer integrations, reconfiguring inventory workflows, and absorbing a productivity dip that lasts months. Most HME operators stay on a platform for five to ten years, whether they like it or not, because the cost of leaving feels too high.
That makes the selection decision consequential in a way most enterprise software decisions are not. Choose a platform with weak claims scrubbing, and you will spend the next decade managing a 15 to 18 percent denial rate. Choose a platform with no API surface, and you will be locked out of every AI and automation tool that comes to market. Choose a platform that has not meaningfully updated its Medicare Advantage coverage rules library, and your billing team will manually correct MA-related errors on every third claim.
The HME software market in 2026 looks very different from 2020. Several legacy platforms have added AI-adjacent features of variable quality. Cloud-native competitors have matured. The clearinghouse landscape has consolidated. AI automation layers, built on top of the core platform rather than inside it, have emerged as a real option for operators who need more than the platform can deliver natively.
This guide is written for the HME operator making a platform decision or a renewal decision in 2026. It covers what the best platforms do, where the gaps are, and how to evaluate what you are actually buying, not what the sales deck says you are buying.
What Does This Guide Cover?
- What HME software actually does and what the best platforms do that the rest do not
- The 8 non-negotiable features for 2026
- The 7 red flags to avoid in HME software selection
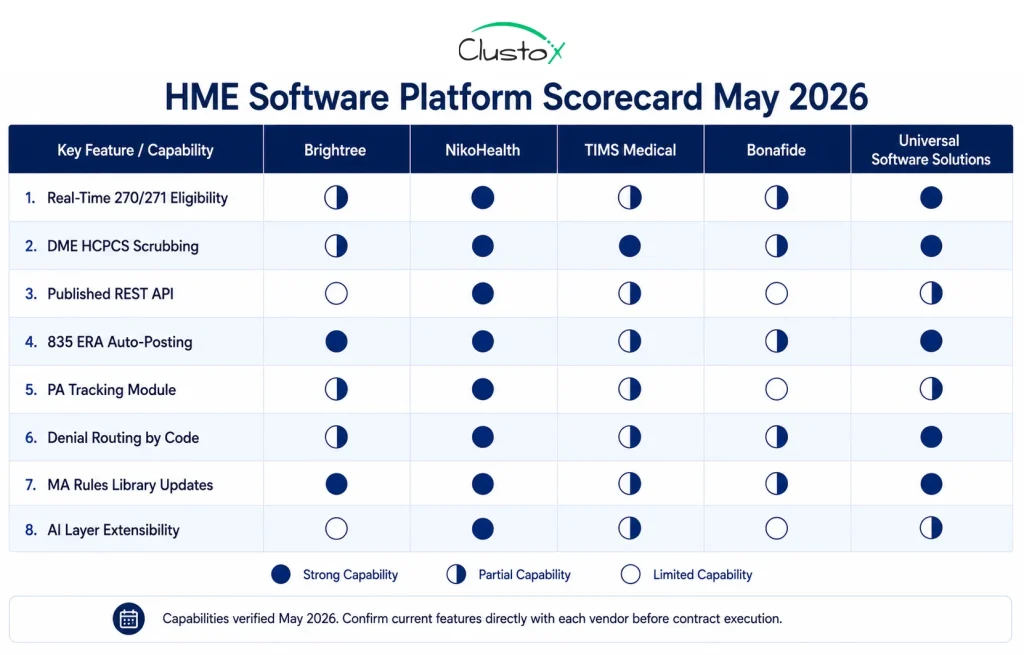
- Platform comparison: Brightree, NikoHealth, TIMS Medical, Bonafide, and Universal Software Solutions
- How AI layers extend what HME software can do and what they require
- A structured three-tier evaluation checklist for operations and billing decision-makers
- Eight frequently asked questions covering the most common buyer concerns
What Is HME Software and What Should It Do in 2026?
HME software, short for home medical equipment software, is the operational platform that manages the end-to-end workflow of an HME or DME business. That scope includes patient and referral management, inventory and delivery tracking, insurance eligibility verification, claim submission and denial management, compliance documentation, and operational reporting.
In 2026, the baseline expectation for HME software has moved well beyond what most platforms were originally designed to deliver.
The gap between what operators need and what legacy platforms provide is widest in 6 areas.
- Patient intake: Operators need automated referral parsing, real-time eligibility confirmation, and same-day order qualification. Most legacy platforms still require manual data entry, with a basic eligibility look-up tool added on rather than built in.
- Insurance verification: Operators need real-time 270/271 EDI with HCPCS-level benefit parsing. Legacy platforms typically offer 270/271 support but default to batch processing overnight rather than real-time response.
- Prior authorization: Operators need PA requirement detection, automated submission routing, and status tracking in a single workflow. Legacy platforms typically rely on manual PA tracking in a separate module or a spreadsheet running alongside the main system.
- Claims scrubbing: Operators need DME-specific HCPCS and modifier validation, payer-specific edits, and denial prediction scoring. Legacy platforms often use generic claim scrubbers with DME configurations added on top, leaving DME-specific modifier errors and rental-versus-purchase rule violations uncaught.
- Denial management: Operators need denial reason code routing, structured appeal workflows, and pattern analytics by payer and code. Legacy platforms offer a denial work queue. Everything after that is manual.
- Reporting: Operators need real-time KPI dashboards and denial root cause reports. Legacy platforms produce static exports and batch reports that lag by a day or more, making it difficult to catch problems before they compound.
What are the 8 Non-Negotiable Features for HME Software in 2026?
These 8 features represent the minimum viable capability set for any HME platform evaluated in 2026. Any vendor that cannot demonstrate these in a live environment, not a pre-recorded walkthrough, should be removed from consideration before pricing discussions begin.
Table of Contents
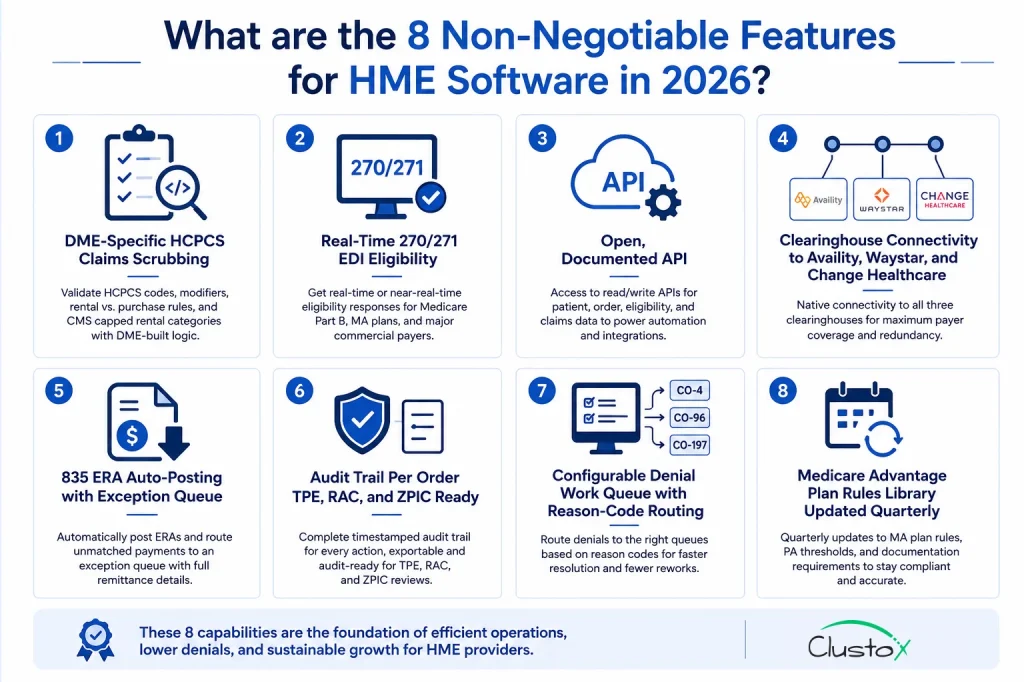
1. DME-Specific HCPCS Claims Scrubbing
The scrubber must understand HCPCS Level II codes, their associated modifiers (KX, GA, GY, GZ, NU, RR, UE), rental versus purchase rules, and CMS capped rental categories. A generic medical billing scrubber adapted for DME is a different product from one built for it. Ask the vendor to run a live demonstration on a power wheelchair claim (K0856) and an oxygen claim (E1390) before you proceed. If they switch to a screen recording or defer to a future session, that response tells you what you need to know.
2. Real-Time 270/271 EDI Eligibility
Batch eligibility, submitted overnight and returned the next morning, is not adequate for modern intake workflows. You need real-time or near-real-time eligibility response for Medicare Part B, your top Medicare Advantage plans, and major commercial payers. A vendor offering only batch 270/271 processing creates a workflow constraint that your intake team will feel on every single order.
3. Open, Documented API
If the platform does not have a published API that allows read and write access to patient records, order data, eligibility results, and claim status, you cannot build automation on top of it. This is the single most important architectural requirement for any operator who plans to use AI tools, automate intake, or integrate with an EHR in the next three years. Ask for the actual API documentation before the demo progresses. Not a description of what the API can do. The documentation itself.
4. Clearinghouse Connectivity to Availity, Waystar, and Change Healthcare
These three clearinghouses handle the majority of DME claim traffic. Native connectivity to all three gives you redundancy when one clearinghouse has an outage, plus flexibility when a payer requires a specific clearinghouse for EDI submission. Confirm which clearinghouse routes which payer category before assuming full payer coverage.
5. 835 ERA Auto-Posting with Exception Queue
Electronic Remittance Advice should post automatically to the patient account and order record without manual intervention. Unmatched payments, where the ERA cannot be automatically reconciled to a specific claim, should route to a clearly labeled exception queue. The exception queue should display the ERA detail alongside the original claim so staff can resolve mismatches efficiently rather than searching across systems.
6. Audit Trail Per Order TPE, RAC, and ZPIC Ready
Every action on every order must be logged with a timestamp and user attribution. That includes eligibility checks, document receipts, claim submissions, ERA postings, denial routings, and appeal submissions. When a Targeted Probe and Educate review, RAC audit, or ZPIC request arrives, you need to produce a complete order history without manual reconstruction.
Platforms that store audit data in exportable formats, not only in-platform views, are meaningfully easier to work with during audit response. CMS guidance on DME audit documentation requirements is available on the CMS website and should inform how your audit trail is structured.
7. Configurable Denial Work Queue with Reason-Code Routing
Not all denial reason codes require the same response. A CO-4 (procedure code inconsistent with modifier) has a different resolution path than a CO-96 (non-covered charge) or a CO-197 (precertification absent).
The denial work queue must route claims to the appropriate staff queue based on the denial reason code, not deposit everything into a single unfiltered list. Ask to see denial routing in action for at least five common denial types during the live demonstration.
8. Medicare Advantage Plan Rules Library Updated Quarterly
Each Medicare Advantage plan maintains its own HCPCS coverage policies, PA thresholds, and documentation requirements. These change annually and sometimes mid-year. A platform with a static MA rules library becomes an increasing liability as your MA patient volume grows.
Ask the vendor how often the MA rules library is updated, who is responsible for maintaining it, and what the process is when a plan changes its coverage policy outside the annual cycle.
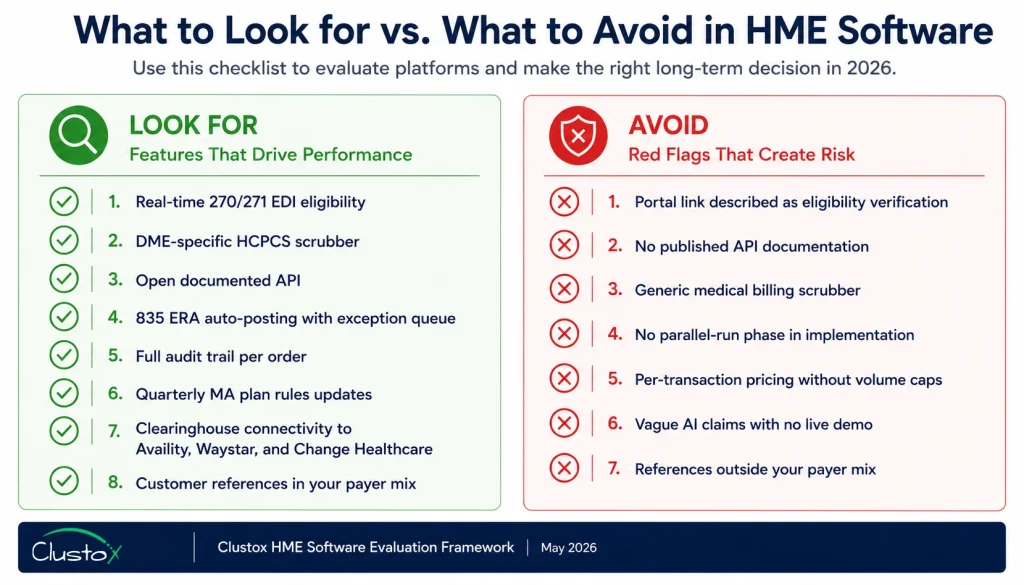
What Red Flags Should You Watch for When Selecting HME Software?
These are the patterns that HME operators identify as warning signs, either in product demonstrations, contract negotiations, or the first year of live use.
Each one represents a gap that will cost your operation time, revenue, or both.

Red Flag 1: Eligibility Verification That Is Actually a Portal Link
Some platforms advertise eligibility verification as a feature, but what they deliver is a link to the payer’s eligibility portal that opens in a browser window for your coordinator to read manually.
That is manual verification described as software functionality. Real eligibility automation submits a 270 transaction and parses the 271 response automatically. It does not open a web page and expects your staff to transcribe the result.
Red Flag 2: No Published API Documentation
If a vendor cannot point you to public API documentation or offers only a custom integration service at an additional cost, you are evaluating a closed platform. Closed platforms cannot be automated, cannot connect to AI tools, and cannot integrate with modern EHR systems.
This constraint will affect your operation for the entire contract term, which is typically five to ten years in the HME space.
Red Flag 3: Generic Claim Scrubbing Rules Not Built for DME
Ask the vendor directly whether the scrubber was built specifically for HCPCS Level II and DME billing rules, or whether it is a general medical billing scrubber with some DME configurations added on top. The answer matters significantly. Generic scrubbers miss DME-specific modifier requirements, rental versus purchase rule violations, and HCPCS code and diagnosis code pairing requirements. Each miss is a preventable denial.
Red Flag 4: Implementation Plans Without a Parallel-Run Phase
Any HME software implementation that does not include a structured parallel-run period, where the new platform runs alongside the existing system before cutover, is taking a material risk with your revenue cycle.
During the parallel run, you validate that eligibility results match, claim submissions are correct, and ERA posting is accurate before the old system is retired. Skipping this phase to accelerate go-live is a consistent predictor of revenue cycle disruption in the first 60 days after cutover.
Red Flag 5: Per-Transaction Pricing Without Volume Caps
Some HME platforms price eligibility checks, claim submissions, or document storage on a per-transaction basis. This structure sounds reasonable until your volume grows and transaction fees become a significant share of your total software cost.
Always model the total cost of ownership at 1.5 times and 2 times your current order volume before signing. If volume caps or tiered pricing are not in the contract, negotiate them in before execution.
Red Flag 6: Vague AI Claims With No Working Demonstration
Every major HME software vendor now includes the word AI in their marketing materials. The meaningful question is what the AI actually does, where it operates in the workflow, and whether you can see it working on your specific claim types in a live environment.
Phrases like intelligent automation or machine learning-powered insights without specifics typically describe a rules engine with a modern label. Ask for a live demonstration of the AI feature on a power wheelchair claim and an oxygen claim. If the vendor cannot show it working in real time, the feature is not ready for production use.
Red Flag 7: No Customer References in Your Payer Mix
HME billing complexity varies significantly by payer mix. A vendor with strong Medicare Part B references but limited Medicare Advantage experience, or strong commercial payer references but no Medicaid history, may have gaps that will not surface until your operation is live on the platform.
Ask for three customer references whose payer mix is similar to yours, not the three most impressive names on the vendor’s reference list.
How Do AI Layers Change the HME Software Decision in 2026?
The most important shift in the HME software landscape in 2026 is not happening inside the platforms. It is happening in the AI automation layers that sit on top of the core platform via API and extend its capabilities in ways the platform has not built natively.
This shift changes the evaluation framework in two concrete ways. First, platform API quality becomes a make-or-break criterion. If the platform has a weak or undocumented API, you cannot connect AI automation tools regardless of what those tools offer.
Open, documented, REST-based APIs with webhook support are no longer optional features; they are the prerequisite for any automation investment.
Second, native AI features matter less than API extensibility. A platform with a strong API and limited native AI can be more valuable than one with branded AI features and a closed architecture because you can connect the tools that actually work for your operation.
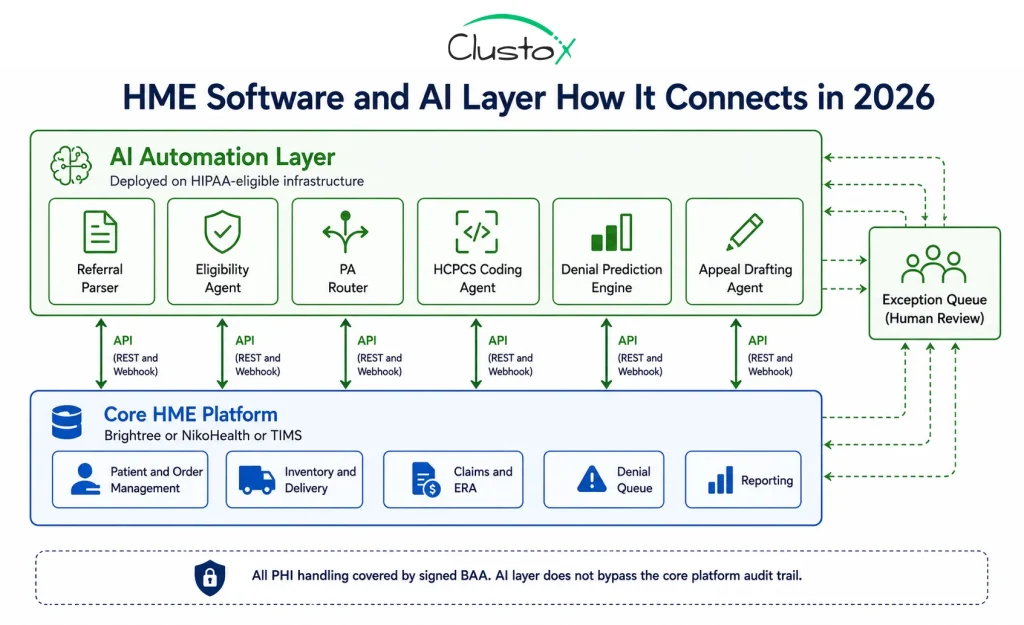
What Can AI Layers Currently Do Well on Top of HME Platforms?
Referral parsing and intake automation: LLM-based document parsers read fax, HL7, and PDF referrals and populate Brightree or NikoHealth automatically, eliminating manual data entry for structured referral types.
Real-time eligibility agents: Eligibility agents run 270/271 EDI queries at the moment a referral arrives rather than waiting for a billing staff member to initiate the check. A task that previously took 18 to 22 minutes per order becomes a sub-minute automated step, per AAHomecare’s 2023 Operational Survey.
Prior authorization routing: Agents check the CMS prior authorization program list and payer-specific requirements, submit the PA request to the payer portal or an electronic PA platform, and track status without a coordinator managing each case manually.
HCPCS code and modifier suggestion: LLM-assisted coding reviews the referral, diagnosis, and clinical notes to suggest the correct HCPCS code and required modifiers before the claim is created. This reduces the volume of modifier errors that generate preventable denials at the claim submission stage.
Denial prediction and pre-submission review routing: Claims are scored for denial risk before submission. High-risk claims route to a review queue rather than submitting and failing, which reduces rework costs significantly.
Automated appeal drafting: Appeal letters are drafted with LCD and NCD citations pulled from the CMS coverage database, reducing appeal drafting time from 45 to 60 minutes per case down to under 10 minutes for standard denial types.
What Can AI Layers Not Handle Yet in HME Operations?
Medicare Advantage edge cases remain a consistent limitation. Each MA plan has its own HCPCS coverage policies, PA thresholds, and documentation requirements. Automated agents handle the standard eligibility check and flag orders for specialist review when the plan’s rules fall outside standard parameters. They cannot resolve every MA coverage dispute independently.
LMN content quality is a hard limit for AI automation. A documentation outreach agent can request a Letter of Medical Necessity and confirm that a document was received. It cannot verify that the LMN’s clinical content meets the payer’s medical necessity criteria. That review remains a human responsibility and a critical one; a technically complete but clinically insufficient LMN is an audit risk under TPE and RAC review.
Medicaid state-specific billing rules require ongoing manual configuration. Medicaid programs are administered at the state level, and DME coverage rules vary significantly across states.
Automated eligibility handles the standard 270/271 transaction, but state-specific PA requirements, rate schedules, and documentation standards need configuration that must be maintained as Medicaid policies change.
What Results Are HME Operators Seeing After Platform and AI Improvements?
The figures below combine published industry benchmarks with operator-reported outcomes from HME and DME providers who implemented platform upgrades or AI automation layers during 2024 and 2025. Results vary by payer mix, starting denial rate, and implementation quality.
Claims and Denial Rate Outcomes
- First-pass claim denial rate: The industry baseline sits at 15 to 18 percent, per the HFMA Revenue Cycle Benchmarking Report 2023. Operators who address eligibility errors, HCPCS coding gaps, and documentation failures through platform and AI improvements consistently reach 7 to 10 percent within 6 to 12 months.
- Eligibility error denial rate: The baseline for eligibility-driven denials is 8 to 12 percent of claims, per HFMA DME benchmark cohort data. Operators using real-time 270/271 eligibility with HCPCS-level benefit parsing report this falling to 2 to 4 percent after full implementation.
- Appeal win rate: Standard appeal win rates sit at 40 to 55 percent across the DME industry. Operators using structured appeal templates with LCD and NCD citations consistently reach 60 to 75 percent win rates, per Clustox client composite data (2024 to 2025, anonymized).
- Cost to collect per claim: The baseline cost to collect sits at 8 to 14 dollars per claim. Operators who reduce denial rework cycles and automate appeal drafting report 5 to 9 dollars per claim, per HFMA revenue cycle benchmark data.
Operational Efficiency Outcomes
- Intake-to-fulfillment time: The industry average for intake-to-fulfillment time is 48 to 72 hours for operations running manual workflows, per AAHomecare’s 2023 Operational Survey. Operators running the full automated intake workflow including real-time eligibility and automated documentation outreach reach under 4 hours for straight-through eligible referrals.
- Staff hours per intake order: Manual intake consumes 45 to 90 minutes of staff time per order. Operators using automated intake report 10 to 15 minutes per order, with that time spent on exception review rather than data entry and eligibility calls.
- Orders processed per FTE per month: The industry baseline is 80 to 110 orders per full-time equivalent staff member. Operators with automated intake and claims workflows report 200 to 280 orders per FTE the same headcount handling more than twice the volume.
- Days in accounts receivable: The industry average for DME DAR sits at 45 to 65 days. Operators who improve ERA auto-posting and denial resolution speed consistently reach 32 to 45 days, per HFMA revenue cycle benchmark data.
What Does a Full HME Software Implementation Actually Look Like?
HME software implementations are complex enough that the implementation plan deserves as much scrutiny as the software features. The following phases reflect a mid-size HME operation processing 200 to 500 orders per month, switching from a legacy platform to Brightree or NikoHealth with an AI automation layer added. Total expected timeline: 16 to 24 weeks.
What Prerequisites Must Be in Place Before Implementation Starts?
- Platform API access confirmed: Most enterprise and mid-market licenses include API access. Confirm this with your account manager before implementation begins, not after the contract is signed.
- Clearinghouse enrollment for 270/271 EDI: Required for real-time eligibility. If your operation currently relies on manual portal calls for eligibility, clearinghouse enrollment is the first prerequisite to resolve before implementation planning begins.
- Fax-to-digital routing: If your operation receives referrals by fax, and most do a fax digitization layer such as eFax or Kno2, routes inbound faxes to a monitored digital queue that the referral parser can process automatically.
- HIPAA-compliant infrastructure for the AI layer: Signed Business Associate Agreements with all infrastructure vendors, including the AI platform provider, document storage provider, and SMS provider, must be in place before patient data touches any AI system.
What Does the Implementation Timeline Look Like Phase-by-Phase?
- Discovery and data audit (Weeks 1 to 3): Map all current workflows, payer contracts, and integration points. Audit patient and order data for migration quality before a single record is moved to the new platform.
- Data migration and validation (Weeks 2 to 5): Migrate patient records, order history, and the document archive. Validate completeness and accuracy before moving forward to platform configuration.
- Payer and clearinghouse setup (Weeks 3 to 7): Configure payer contracts, fee schedules, clearinghouse connections, and EDI enrollment. This phase often takes longer than vendors estimate when payer credentialing delays arise.
- Platform configuration (Weeks 4 to 8): Set up HCPCS scrubbing rules, denial routing queues, inventory workflows, and user roles. Configuration quality in this phase directly determines the clean claim rate after go-live.
- AI layer integration (Weeks 5 to 11, if applicable): Connect automation agents to the platform API. Configure eligibility agents, PA routing logic, and intake parsing for your specific referral source mix.
- Staff training (Weeks 9 to 11): Role-specific training for billing, intake, inventory, and operations staff. This means separate sessions for different teams, not a single all-hands walkthrough that leaves each group with gaps.
- Parallel run (Weeks 12 to 14): Both systems run simultaneously. Outputs are validated side-by-side before cutover. This phase cannot be skipped without accepting material risk to the revenue cycle at go-live.
- Cutover and stabilization (Weeks 15 to 20): The legacy system is retired. Exception handling procedures are documented. Stabilization support from the vendor should be defined contractually at a named contact level, not routed through a general support queue.
What Should Be on Your HME Software Evaluation Checklist?
The checklist below is structured across three tiers. Work through Tier 1 completely before moving to Tier 2. Any platform that cannot satisfy Tier 1 criteria in a live demonstration should not advance to the pricing stage.
Tier 1: What Must Every Platform Demonstrate Before You Proceed?
- Real-time 270/271 EDI eligibility demonstrated live on your top payer types, not described in a slide or shown in a recording
- DME-specific HCPCS scrubber live demonstration on a power wheelchair (K0856) and an oxygen (E1390) claim with modifier requirements shown
- Published, documented REST API: actual documentation provided before the contract stage, not after signing
- 835 ERA auto-posting with exception queue asks specifically how unmatched payments are surfaced and what the resolution workflow looks like
- Clearinghouse connectivity to Availity, Waystar, and Change Healthcare confirms which payer categories route through which clearinghouse
- Audit trail per order exportable for TPE, RAC, and ZPIC response, not only viewable within the platform interface
- HIPAA compliance documentation, SOC 2 Type II certification, and willingness to execute a BAA before contract signing
- Named customer references in your payer mix at least three, contactable, with comparable payer complexity to your operation
Tier 2: What Differentiates Strong Platforms from Average Ones?
- Prior authorization tracking is integrated into the claims workflow, not maintained in a separate module or spreadsheet
- Medicare Advantage plan rules library updated at least quarterly with a documented update process for mid-year plan changes
- Configurable denial routing by reason code, not a single unfiltered denial queue
- Denial prediction scoring that runs before claim submission rather than after a rejection
- Patient SMS or email intake portal with HIPAA-compliant document upload capability
- Webhook support for real-time event-driven integrations with third-party tools
- EHR integration capability via HL7 FHIR with Epic, Cerner, or athenahealth
Tier 3: What Should You Evaluate If Automation Is a Near-Term Priority?
- LangGraph-compatible or equivalent agentic AI orchestration support, documented and demonstrable by the vendor
- Native denial pattern analytics with root cause reporting by payer, HCPCS code, and referring provider
- Automated appeal drafting with LCD and NCD citation integration, pulling directly from CMS coverage database
- Voice agent or LLM-based referral parser for intake automation at the fax or phone referral stage
Frequently Asked Questions About HME Software
What Is the Difference Between HME Software and DME Software?
HME and DME are used interchangeably in both clinical and software contexts, and the platforms that use either label typically cover the same product category. HME is the broader clinical term covering oxygen, CPAP, wheelchairs, hospital beds, and other equipment used in the home. DME is the CMS billing category that defines which equipment qualifies for Medicare reimbursement under Part B. The distinction matters more in regulatory and clinical contexts than it does in software selection.
How Much Does HME Software Cost?
HME software pricing varies significantly by platform, operation size, and contract structure. Enterprise platforms such as Brightree and NikoHealth typically price on a per-location or per-user basis, with annual contract values ranging from 30,000 to 150,000 dollars or more for mid-size operations. Smaller platforms such as TIMS Medical and Universal Software Solutions have lower price points, often 10,000 to 40,000 dollars annually, with correspondingly fewer features. Implementation costs covering data migration, configuration, and training add 15,000 to 80,000 dollars depending on complexity. AI automation layers carry separately priced implementation and ongoing licensing costs. Always model total cost of ownership at 1.5 times your current order volume before signing any contract.
Is Brightree the Best HME Software?
Brightree is the market-share leader for mid-to-large HME and DME operations, and its feature set is the most complete of the major platforms. Whether it is the right choice for a specific operation depends on order volume and growth trajectory, payer mix complexity, API integration requirements, budget, and whether the operation plans to add an AI automation layer. NikoHealth is a strong alternative for cloud-native operations that prioritise API extensibility. TIMS Medical works well for smaller operators with simpler billing needs. The best platform is the one your team can operate effectively and that supports your automation roadmap.
What Is the Biggest Mistake HME Operators Make When Buying Software?
The most common mistake is evaluating the platform based on the sales demonstration rather than against live use cases. Vendors demonstrate their product under ideal conditions with clean data, standard claim types, and fast payer connections. Gaps surface in edge cases: a Medicare Advantage claim with a non-standard modifier requirement, a fax referral with handwritten clinical notes, or a payer portal timeout during batch eligibility. Insist on a proof-of-concept using your actual top-10 payer types before signing, and speak with references whose operations are similar to yours.
Do I Need a Separate AI Tool, or Does HME Software Include AI?
Most HME software platforms include some AI-adjacent marketing language describing rules-based claim scrubbing as intelligent or denial reporting as AI-powered. Genuinely useful AI capabilities, LLM-based referral parsing, agentic eligibility verification, denial prediction scoring, and automated appeal drafting are generally not built natively into core HME platforms as of 2026. They are delivered as AI automation layers built on top of the platform via API. If AI automation is a priority for your operation, evaluate the platform's API quality first. Then evaluate the AI tools that connect to it.
How Long Does HME Software Implementation Take?
A full HME software implementation covering data migration, payer and clearinghouse setup, platform configuration, staff training, and parallel run takes 16 to 24 weeks for a mid-size operation processing 200 to 500 orders per month. Smaller operations with simpler payer mixes can complete implementation in 8 to 12 weeks. Adding an AI automation layer adds 6 to 10 weeks. Implementations that eliminate the parallel-run phase to accelerate go-live consistently generate revenue cycle disruption in the first 30 to 60 days after cutover.
What Questions Should I Ask HME Software Vendors Before Signing?
Ten questions worth asking before any HME software contract:
Can I read your API documentation now, before we proceed to the next stage of evaluation?
Final Thoughts
Most HME operators do not switch platforms because the software is bad. They stay on platforms that are costing them claims revenue, staff time, and growth capacity because the switching cost feels higher than the status quo. That calculation is often wrong, but understandable, because the real cost of the wrong platform is distributed across thousands of small inefficiencies that never appear on a single line of a profit and loss statement.
A 15 to 18 percent denial rate does not appear as a software cost on the books. It shows up as billing team overtime, write-offs at month-end, and a denial queue that never empties. A 48-hour intake process does not look like a platform limitation. It looks like patient dropout and referral relationships cool quietly over time. These are software problems with operational consequences, and the right platform, properly implemented, addresses them at the source.
The eight non-negotiable features in this guide represent the baseline for what HME software should deliver in 2026. If the current platform cannot demonstrate real-time eligibility, an open API, and configurable denial routing in a live environment, those are gaps worth quantifying against actual claim volume and denial rate before the next renewal decision.
The seven red flags are equally useful as renewal criteria. A platform with a closed API, a generic scrubber, or a static MA rules library will compound those constraints as MA patient volume grows and as AI automation tools become standard practice across the HME market.