
Three years ago, automating DME workflows was a competitive advantage. Only the largest provider groups were doing it. Today, the math has shifted. Providers running manual eligibility checks, prior authorizations, and denial management are absorbing costs that their automated competitors have already eliminated.
The pressure is coming from every direction at once. CMS has expanded prior authorization requirements to more HCPCS code categories. Medicare Advantage and commercial payers are denying claims at rates that were unthinkable five years ago.
Billing staff turnover is at a decade high. And competitive bidding has compressed reimbursement margins to the point where operational inefficiency is a direct threat to viability.
It is an operations article. The DME providers making the most progress in 2026 are not the ones with the most sophisticated AI. They are the ones who identified their highest-cost manual workflows and replaced them with Agentic AI agents that integrate directly into Brightree or NikoHealth.
This article explains exactly what those workflows are, what automation looks like in practice, what the real numbers show, and what limits still exist. If you are a COO, Director of Billing, or VP of Operations, this is the information you need to decide whether and where to move.
What Is Driving the DME Industry’s Shift to Automation in 2026?
Five forces are converging this year. Each one, on its own, is manageable. Together, they make manual operations financially unsustainable for most mid-size DME providers.
Why are CMS prior authorization requirements expanding in 2026?
CMS extended its prior authorization program for DME to additional product categories in late 2025. The agency’s expanded list now covers more HCPCS codes under oxygen therapy, power wheelchairs, and continuous glucose monitors. Providers who have not automated their prior auth workflows are seeing turnaround times of six to nine days.
The CMS Prior Authorization for Certain Hospital Outpatient Department Services final rule and subsequent DME-specific expansions are documented at CMS.gov (2025).
Table of Contents
Automated prior auth agents built on Agentic AI frameworks like LangGraph can reduce that six-to-nine-day window to under 48 hours. The agent checks coverage criteria, pulls the Letter of Medical Necessity (LMN), matches HCPCS codes to payer-specific rules, and submits electronically without staff intervention.
How is the denial rate trend affecting DME revenue in 2026?
Denial rates across Medicare Advantage and commercial payers climbed to an average of 12 to 15 percent for DME claims in 2025, according to AAHomecare’s 2025 industry operations survey (2025). For a provider billing $10 million annually, that translates to $1.2 to $1.5 million in revenue held at risk.
Most soft denials, those triggered by missing documentation, incorrect HCPCS codes, or eligibility mismatches, are recoverable. But recovery requires fast action. Manual denial management teams typically take 18 to 22 days to file an appeal. Automated denial management agents using RAG (Retrieval-Augmented Generation) can draft an appeal with supporting documentation in under four hours.
What is causing the DME staffing shortage,and why does it matter?
The DME billing workforce has not kept pace with demand. Reimbursement compression from competitive bidding rounds has limited salary budgets. Experienced billers who understand HCPCS coding, LMN requirements, and payer-specific prior auth portals are difficult to hire and harder to retain.
The Healthcare Financial Management Association (HFMA) reports that revenue cycle staff turnover in DME reached 28 percent in 2024, per HFMA’s 2024 Revenue Cycle Benchmarking Report (2024). Every departure resets institutional knowledge of payer quirks and workflow shortcuts.
Agentic AI does not quit. It does not call in sick. It does not need retraining when a payer updates its portal. For eligibility verification alone, replacing manual payer portal lookups with automated agents eliminates the single largest time sink in a DME billing operation.
Where Are DME Providers Losing the Most Revenue to Manual Processes?
The five highest-cost manual workflows in a typical DME operation are listed below. Each one has a documented automation solution available today.
| Workflow | Manual Cost Driver | Automation Impact |
|---|---|---|
| Eligibility verification | 2 to 4 hours per batch per day | Under 10 minutes with API-connected agents |
| Prior authorization | 6 to 9 days average turnaround | Under 48 hours with Agentic AI |
| HCPCS code selection | Frequent errors, documentation gaps | AI code intelligence reduces errors by 60%+ |
| Denial management | 18 to 22 days to appeal filing | Under 4 hours with RAG-powered drafting |
| CPAP re-supply outreach | Low contact rates via manual calls | Voice and SMS agents reach 3x more patients |
Brightree and NikoHealth, the two dominant DME practice management platforms, both support API integration with Agentic AI systems. Providers do not need to replace their existing tech stack to automate these workflows. The automation layer sits on top of the existing system and handles the repetitive, rule-based steps.
How Does Agentic AI Work Inside a DME Operation?
Agentic AI refers to AI systems that take multi-step actions autonomously, make decisions, and interact with external systems, rather than simply generating text responses. Organizations implementing Agentic AI Development Services use these systems to automate complex workflows that traditionally require multiple human touchpoints.
In a DME context, this means an AI agent that can log into a payer portal, check eligibility, pull benefit details, flag coverage gaps, and write those results back to Brightree or NikoHealth, all without a human in the loop.
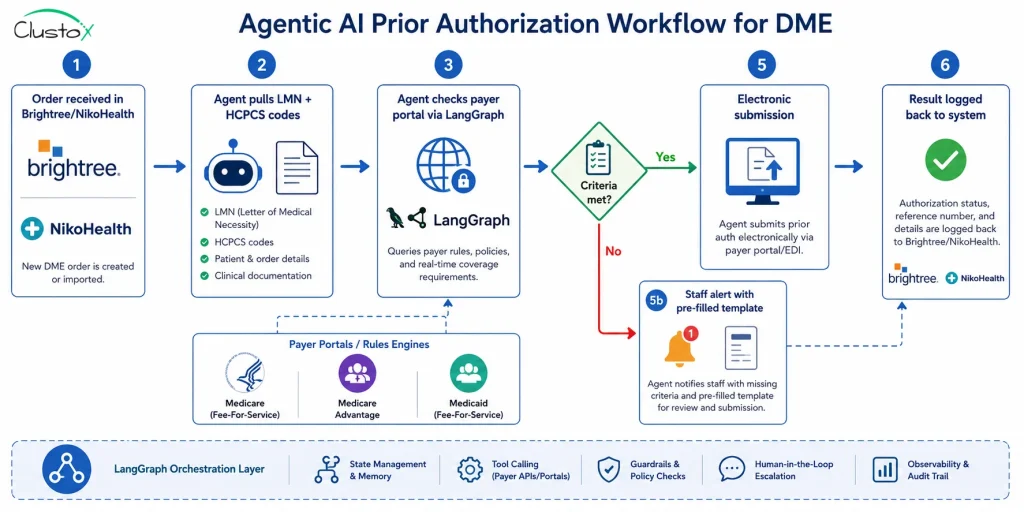
What does a prior authorization automation workflow look like?
- Order is received in Brightree or NikoHealth and tagged for prior auth.
- The Agentic AI agent pulls the patient record, the treating physician’s LMN, and the relevant HCPCS codes.
- The agent checks the specific payer’s prior auth criteria, either via API or portal automation using LangGraph-based orchestration.
- If criteria are met, the agent submits the request electronically and logs the confirmation number.
- If documentation is missing, the agent flags the case, identifies the gap, and routes it to staff with a pre-filled request template.
- Approvals and denials are captured and fed back into the DME management system automatically.
The staff role shifts from data entry and portal navigation to exception handling. A team that previously processed 80 prior auth requests per day manually can handle 300 or more with the same headcount when an agent handles steps 1 through 5.
How does denial management automation work in practice?
When a claim is denied, the agent receives the denial reason code from the payer. It cross-references the reason code against a knowledge base of successful appeal strategies using RAG. The agent drafts an appeal letter, pulls the supporting documentation from the patient record, and routes the package to a billing staff member for one-click submission.
The staff member reviews, approves, and submits. Total staff time is under 10 minutes per case instead of the 45 to 90 minutes required for manual drafting.
This is not theoretical. Clustox has deployed denial management agents for DME providers running Brightree that recover 18 to 27 percent of soft denials that would otherwise be written off.
What Do the Real Numbers Look Like for DME Automation in 2026?
Snackable Data Points
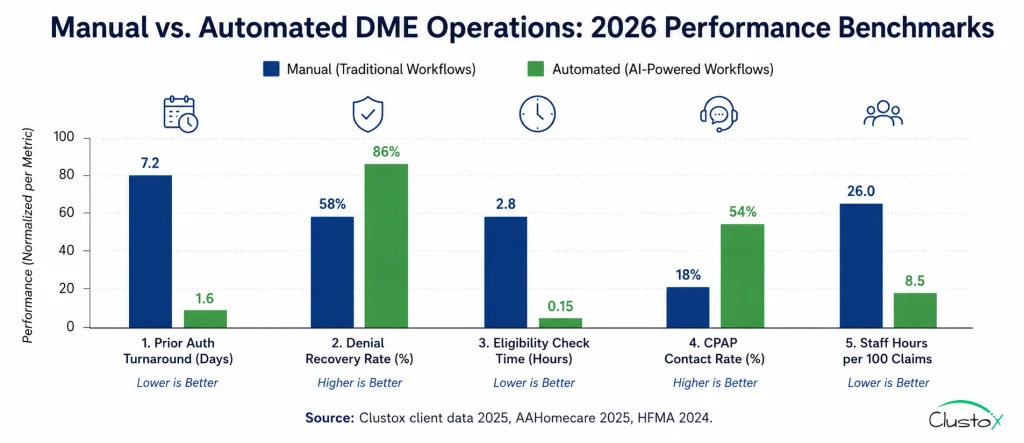
Prior auth turnaround drops from 6.2 days to 1.8 days on average with Agentic AI, per Clustox client deployments (2025).
Denial recovery rates increase by 18 to 27 percent when RAG-powered appeal drafting is introduced, per Clustox internal data (2025).
Eligibility verification time drops from 3.5 hours per day to under 20 minutes with API-connected agents, per AAHomecare benchmarks (2025).
CPAP re-supply contact rates increase by 200 to 300 percent using AI voice and SMS agents vs. manual outbound calls, per Clustox client data (2025).
DME billing staff turnover reached 28 percent in 2024, per HFMA’s Revenue Cycle Benchmarking Report (2024).
What is a realistic ROI timeline for DME automation?
The answer depends on billing volume and current denial rates. A provider billing $5 million annually with a 12 percent denial rate is sitting on $600,000 of at-risk revenue. If an automation layer recovers half of soft denials and cuts prior auth delays that hold up claim submission by two to three days, the cash flow improvement is measurable within 90 days.
Most Clustox deployments reach full ROI within six months. The fixed cost of a 48-hour AI Readiness Audit is the starting point. That audit maps which workflows will generate the fastest return and produces a prioritized build plan.
What are the Limits of DME Automation Right Now?
Automation is not a solution for every DME workflow problem. Here is where current Agentic AI systems hit their limits.
- Ambiguous medical necessity: Complex medical necessity reviews still need human judgment. When a payer’s criteria are ambiguous or documentation is genuinely insufficient, an agent cannot manufacture clinical evidence. A human reviewer is required.
- Unstable payer portals: Payer portal inconsistency. Some smaller regional payers and Medicare Advantage plans do not have stable portals or APIs. Agent reliability drops when portal layouts change without notice.
- Patient escalation: High-touch patient situations. CPAP resupply voice agents work well for routine outreach but should route to a human agent when a patient expresses confusion, frustration, or a complex clinical question.
- HIPAA architecture: HIPAA compliance is non-negotiable. Any Agentic AI system handling PHI must be architected with HIPAA-compliant infrastructure. This means encrypted data transit, audit logging, access controls, and a signed BAA with every vendor in the stack. AWS Bedrock supports HIPAA-eligible workloads. Not every LLM provider does.
- Implementation effort: Initial workflow mapping takes time. The first 30 to 60 days of an automation deployment are invested in documenting current-state workflows, configuring integrations with Brightree or NikoHealth, and running parallel testing. Operators should plan for this before expecting results.
How Should DME Operators Evaluate an Automation Partner in 2026?
Not every vendor selling AI to DME providers understands the workflow complexity involved. Use this checklist when evaluating.
| Evaluation Criterion | What to Look For |
|---|---|
| DME-specific experience | Can they name your HCPCS code categories, your audit exposure (TPE, RAC, ZPIC, UPIC), and your current payer mix? |
| Integration depth | Native Brightree or NikoHealth integration vs. manual CSV export. Ask for the integration architecture diagram. |
| HIPAA compliance documentation | Signed BAA is ready on day one. Ask about their data retention and encryption standards. |
| Workflow audit methodology | Do they map your current-state workflows before recommending automation? If not, walk away. |
| Denial-specific capability | Can the agent generate appeal letters, not just flag denials? Ask for a demo with a real CMS denial reason code. |
| Voice agent quality | For CPAP re-supply, listen to a live call sample. Generic voice agents sound like spam calls and hurt contact rates. |
| ROI model transparency | Can they show a model specific to your billing volume, denial rate, and current staffing? Generic ROI claims are a red flag. |
| Reference accounts | Ask for three DME operators of similar size with live deployments, not pilots. |
Conclusion
The DME operators who are ahead in 2026 made one decision differently from everyone else. They stopped treating automation as a future project and mapped their current-state workflows against specific, available tools.
The gap between a manual operation and an automated one is not a technology gap. It is a workflow map gap. Once you know exactly where staff time is going, where denials are originating, and where prior auth delays are holding up cash flow, the automation build plan writes itself.
The five workflows that deliver the fastest ROI for most DME providers are eligibility verification, prior authorization, HCPCS code validation, denial management, and CPAP re-supply outreach. All five have proven Agentic AI solutions. All five integrate with Brightree and NikoHealth. None of them require replacing your existing tech stack.
The honest reality is that implementation takes 45 to 90 days for a focused deployment. It requires upfront workflow documentation and parallel testing. It is not a plug-and-play product. But providers who have gone through it report that the first 90 days post-launch produce measurable cash flow improvement in denial recovery and prior auth turnaround time.
The starting point is a workflow audit. Map what your team actually does today across those five processes. Quantify the time spent, the error rates, and the revenue held at risk by delays. That audit is the foundation for every automation decision that follows.
Frequently Asked Questions
Does DME automation require replacing Brightree or NikoHealth?
No. Agentic AI systems integrate with Brightree and NikoHealth via API. Your existing practice management system stays in place. The automation layer connects to it, reads order data, writes back results, and handles external payer interactions. Most providers see no change to their core system configuration during implementation.
Is Agentic AI HIPAA compliant for DME workflows?
HIPAA compliance depends on how the system is architected, not on AI itself. A properly built system uses encrypted data transit, access controls, audit logging, and a signed Business Associate Agreement (BAA) with every vendor in the stack. AWS Bedrock supports HIPAA-eligible workloads. Providers should require a signed BAA and a written security architecture summary from any automation vendor before granting PHI access.
Which DME workflows should be automated first?
Prioritize based on revenue impact. For most providers, eligibility verification delivers the fastest ROI because it is high-volume and fully automatable. Prior authorization is second because turnaround time directly affects cash flow. Denial management is third because it recovers revenue already submitted but held. CPAP re-supply outreach is a strong fourth for providers with large CPAP patient populations.
How long does a DME automation implementation take?
A focused deployment targeting one or two workflows, such as eligibility verification and prior auth, typically takes 45 to 90 days from kickoff to live operations. Broader deployments covering denial management, re-supply outreach, and audit preparation take 90 to 180 days. The first step is a workflow audit that maps current-state processes and identifies integration requirements.
What is the risk of a CMS or ACHC audit when using AI workflows?
Properly implemented Agentic AI reduces audit risk by standardizing documentation. Every prior auth submission follows the same criteria-matching process. Every claim has a documented eligibility verification. Every denial has an appeal package with source documentation. ACHC and BOC auditors look for consistent, documented processes. Automation creates that consistency at scale. The risk is not the AI itself but the quality of the workflow design and the accuracy of the underlying data.
Do ZPIC, RAC, and TPE auditors target providers using automated billing workflows?
OIG and CMS audit selection is based on claim patterns, error rates, and statistical outliers, not on whether a provider uses automation. In practice, automated workflows that apply consistent HCPCS code selection and documentation standards tend to produce cleaner claim patterns than manual processes prone to human error. Providers should maintain complete audit trails of all automated decisions as part of their Medicare audit defense documentation.
What does a 48-hour AI Readiness Audit include for DME providers?
A 48-hour AI Readiness Audit from Clustox maps your current-state workflows for the five highest-impact DME processes: eligibility verification, prior authorization, HCPCS code selection, denial management, and re-supply outreach. The output is a prioritized automation roadmap with a specific ROI model tied to your billing volume, denial rate, and current staffing. The audit is fixed-price and delivered in 48 hours from kickoff.
Can voice agents handle CPAP resupply outreach effectively?
Yes, when designed correctly. Generic robocall-style voice agents produce low contact rates and damage patient relationships. AI voice agents trained on DME-specific patient conversations, using natural language and real-time decision trees, consistently outperform manual outreach teams. The key metrics are contact rate, re-supply conversion rate, and patient satisfaction scores. Ask any voice agent vendor to share those three numbers from live DME deployments before signing a contract.
What happens to billing staff when automation is introduced?
Billing staff shift from data entry to exception handling and oversight. The volume of repetitive tasks falls sharply. Staff handle the cases that require human judgment, such as complex medical necessity reviews, patient escalations, and payer disputes that go beyond standard appeals. Most DME operators who automate do not reduce headcount immediately. They redirect existing staff capacity to denial recovery and audit preparation, which are higher-value activities.